

Assessment of PaO₂/FiO₂ for stratification of patients with moderate and severe acute respiratory distress syndrome
- PMID: 25818272
- PMCID: PMC4386240
- DOI: 10.1136/bmjopen-2014-006812
Assessment of PaO₂/FiO₂ for stratification of patients with moderate and severe acute respiratory distress syndrome
Abstract
Objectives: A recent update of the definition of acute respiratory distress syndrome (ARDS) proposed an empirical classification based on ratio of arterial partial pressure of oxygen to fraction of inspired oxygen (PaO₂/FiO₂) at ARDS onset. Since the proposal did not mandate PaO₂/FiO₂ calculation under standardised ventilator settings (SVS), we hypothesised that a stratification based on baseline PaO₂/FiOv would not provide accurate assessment of lung injury severity.
Design: A prospective, multicentre, observational study.
Setting: A network of teaching hospitals.
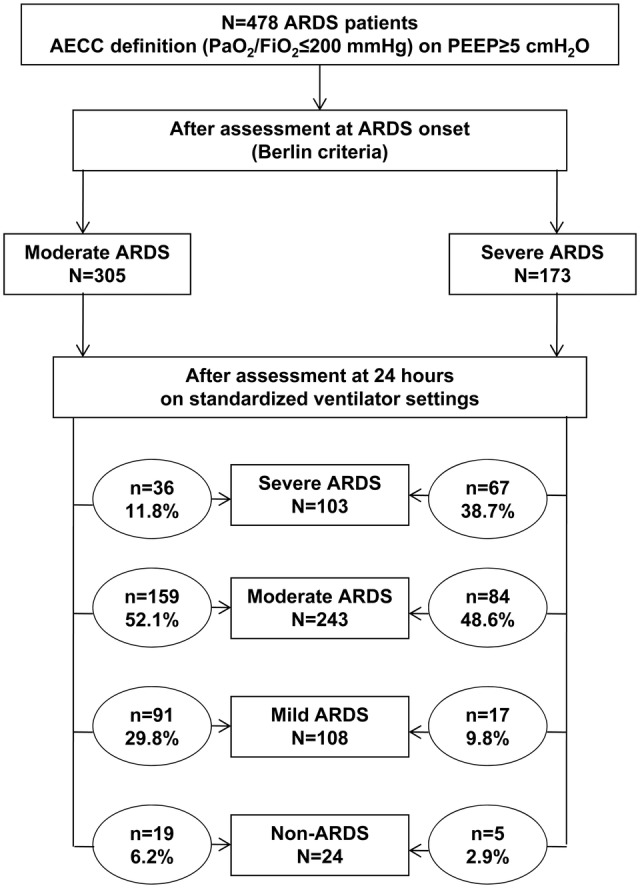
Participants: 478 patients with eligible criteria for moderate (100<PaO₂/FiO₂≤200) and severe (PaO₂/FiO₂≤100) ARDS and followed until hospital discharge.
Interventions: We examined physiological and ventilator parameters in association with the PaO₂/FiO₂ at ARDS onset, after 24 h of usual care and at 24 h under a SVS. At 24 h, patients were reclassified as severe, moderate, mild (200<PaO₂/FiO₂≤300) ARDS and non-ARDS (PaO₂/FiO₂>300).
Primary and secondary outcomes: Group severity and hospital mortality.
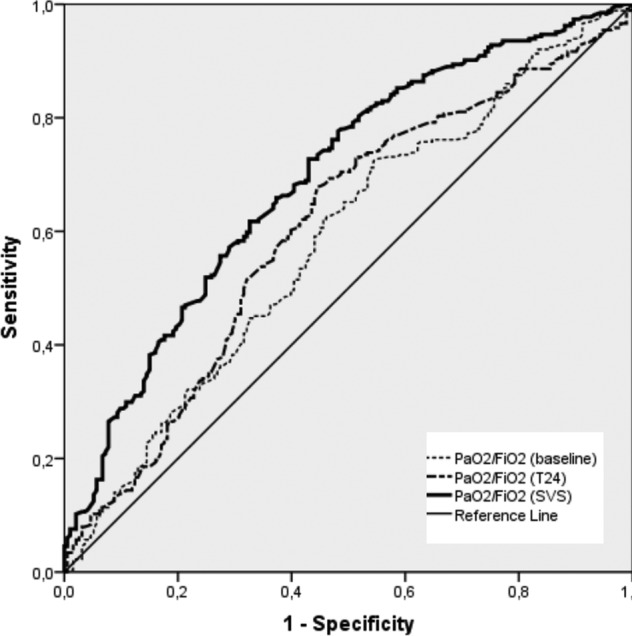
Results: At ARDS onset, 173 patients had a PaO₂/FiO₂≤100 but only 38.7% met criteria for severe ARDS at 24 h under SVS. When assessed under SVS, 61.3% of patients with severe ARDS were reclassified as moderate, mild and non-ARDS, while lung severity and hospital mortality changed markedly with every PaO₂/FiO₂ category (p<0.000001). Our model of risk stratification outperformed the stratification using baseline PaO₂/FiO₂ and non-standardised PaO₂/FiO₂ at 24 h, when analysed by the predictive receiver operating characteristic (ROC) curve: area under the ROC curve for stratification at baseline was 0.583 (95% CI 0.525 to 0.636), 0.605 (95% CI 0.552 to 0.658) at 24 h without SVS and 0.693 (95% CI 0.645 to 0.742) at 24 h under SVS (p<0.000001).
Conclusions: Our findings support the need for patient assessment under SVS at 24 h after ARDS onset to assess disease severity, and have implications for the diagnosis and management of ARDS patients.
Trial registration numbers: NCT00435110 and NCT00736892.
Keywords: RESPIRATORY MEDICINE (see Thoracic Medicine).
Published by the BMJ Publishing Group Limited. For permission to use (where not already granted under a licence) please go to http://group.bmj.com/group/rights-licensing/permissions.
Figures
References
Publication types
MeSH terms
Substances
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous