

Outcomes of Infection-Related Hospitalization according to Dialysis Modality
- PMID: 25818336
- PMCID: PMC4422244
- DOI: 10.2215/CJN.09210914
Outcomes of Infection-Related Hospitalization according to Dialysis Modality
Abstract
Background and objectives: Peritoneal dialysis (PD) is associated with an increased risk of infection-related hospitalization (IRH) compared with hemodialysis. The objective of this study was to compare mortality and overall readmission after an IRH between PD and hemodialysis.
Design, setting, participants, & measurements: This propensity score-matched retrospective cohort study assessed patients undergoing long-term dialysis patients, derived from the Canadian Organ Replacement Register and Régie de l'assurance maladie du Québec, who had at least one IRH between January 2001 and December 2007. Patients were followed until death, kidney transplantation, or end of the study period. To estimate the probability of receiving PD versus hemodialysis, propensity scores were obtained using multivariable logistic regression. Mortality and overall readmission risks after the initial IRH were compared using a Cox survival model.
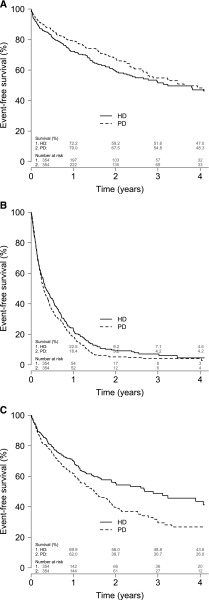
Results: A total of 354 pairs of patients who had at least one IRH were matched for propensity score. During follow-up (median, 1.25 years), 138 hemodialysis patients (24.7/100 patient-years; 95% confidence interval [95% CI], 20.7 to 29.1) and 130 PD patients (21.2/100 patient-years; 95% CI, 17.7 to 25.1) died; 265 hemodialysis patients (144.6/100 patient-years; 95% CI, 127.7 to 163.1) and 299 PD patients (173.2/100 patient-years; 95% CI, 154.1 to 194.0) were readmitted for any cause; and 121 hemodialysis patients (29.7/100 patient-years; 95% CI, 24.7 to 35.5) and 168 PD patients (44.7/100 patient-years; 95% CI, 38.2 to 52.0) were readmitted for an infection. Compared with hemodialysis, PD was not associated with a different mortality risk after an IRH (hazard ratio [HR], 0.87; 95% CI, 0.69 to 1.11). PD was associated with a higher risk of infection-related overall readmission compared with hemodialysis (HR, 1.44; 95% CI, 1.14 to 1.81), but not with the risk of all-cause overall readmission (HR, 1.15; 95% CI, 0.98 to 1.36).
Conclusions: PD was not associated with higher mortality or all-cause overall readmission following an IRH compared with hemodialysis, but PD patients were at higher risk of infection-related overall readmission after IRH. IRHs are associated with significant mortality and overall readmissions. Evaluation of strategies to reduce infections in both hemodialysis and PD recipients are needed to improve patient care and outcomes.
Keywords: ESRD; chronic dialysis; epidemiology and outcomes; mortality; peritoneal dialysis.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- U.S. Renal Data System : USRDS 2011 Annual Data Report: Atlas of Chronic Kidney Disease and End-Stage Renal Disease in the United States, Bethesda, MD, National Institutes of Health, National Institute of Diabetes and Digestive and Kidney Diseases, 2011
-
- James MT, Laupland KB: Examining noncardiovascular morbidity in CKD: Estimated GFR and the risk of infection. Am J Kidney Dis 59: 327–329, 2012 - PubMed
-
- Allon M, Depner TA, Radeva M, Bailey J, Beddhu S, Butterly D, Coyne DW, Gassman JJ, Kaufman AM, Kaysen GA, Lewis JA, Schwab SJ, HEMO Study Group : Impact of dialysis dose and membrane on infection-related hospitalization and death: Results of the HEMO Study. J Am Soc Nephrol 14: 1863–1870, 2003 - PubMed
-
- Allon M, Radeva M, Bailey J, Beddhu S, Butterly D, Coyne DW, Depner TA, Gassman JJ, Kaufman AM, Kaysen GA, Lewis JA, Schwab SJ, HEMO Study Group : The spectrum of infection-related morbidity in hospitalized haemodialysis patients. Nephrol Dial Transplant 20: 1180–1186, 2005 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
