

Combination of eccentric exercise and neuromuscular electrical stimulation to improve quadriceps function post-ACL reconstruction
- PMID: 25819154
- PMCID: PMC4754794
- DOI: 10.1016/j.knee.2014.11.013
Combination of eccentric exercise and neuromuscular electrical stimulation to improve quadriceps function post-ACL reconstruction
Abstract
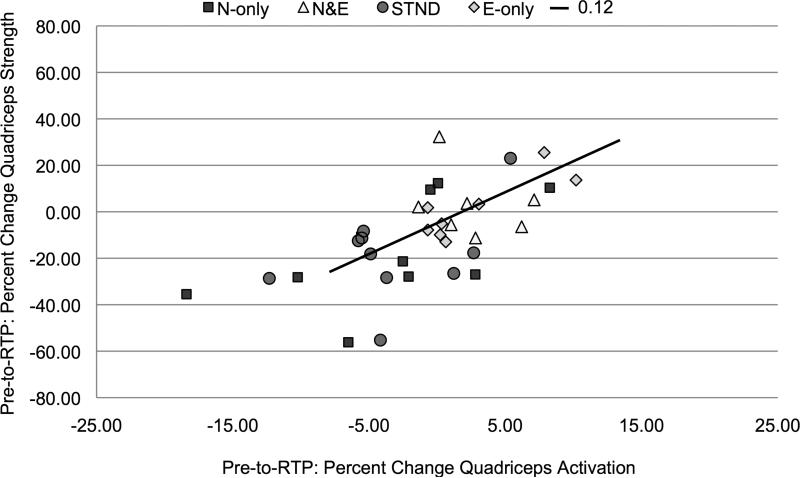
Background: Neuromuscular electrical stimulation (NMES) has been shown to reduce quadriceps activation failure (QAF), and eccentric exercise has been shown to lessen muscle atrophy post-ACL reconstruction. Given that these are two critical components of quadriceps strength, intervention combining these therapies may be effective at reinstituting quadriceps function post-reconstruction. Thus, the aim of this study was to evaluate the effectiveness of a combined NMES and eccentric exercise intervention to improve the recovery of quadriceps activation and strength post-reconstruction.
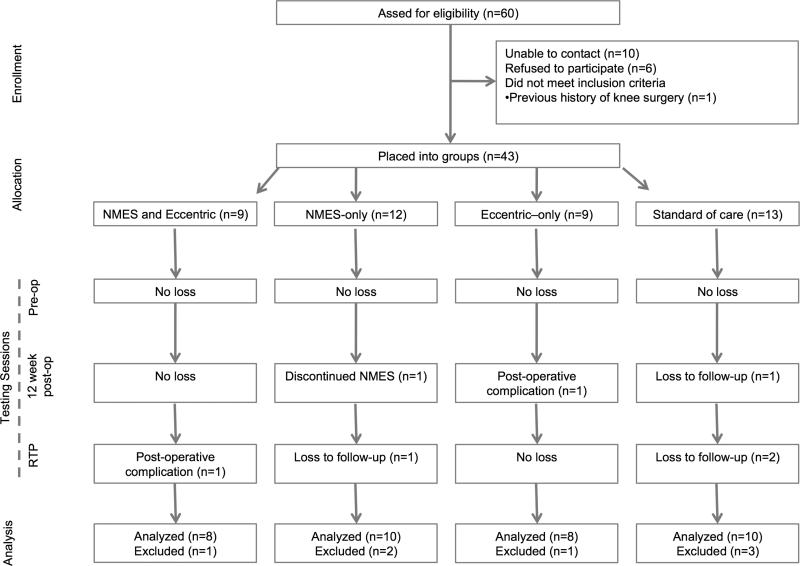
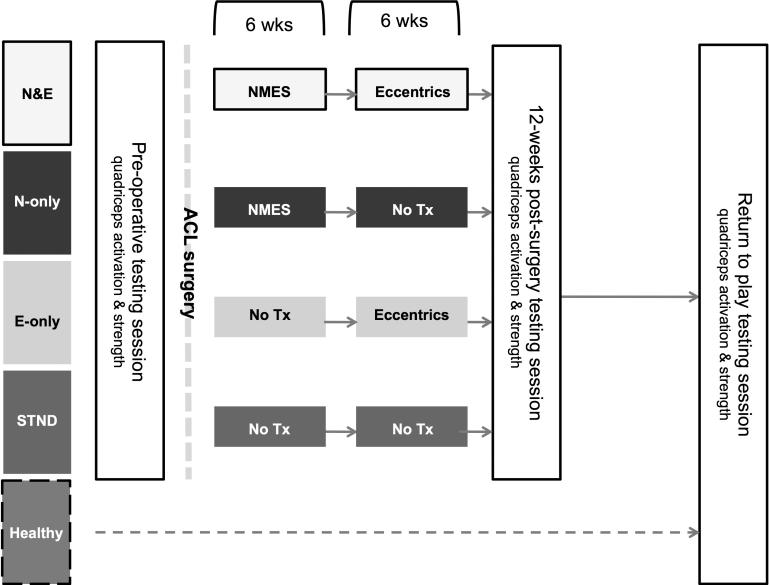
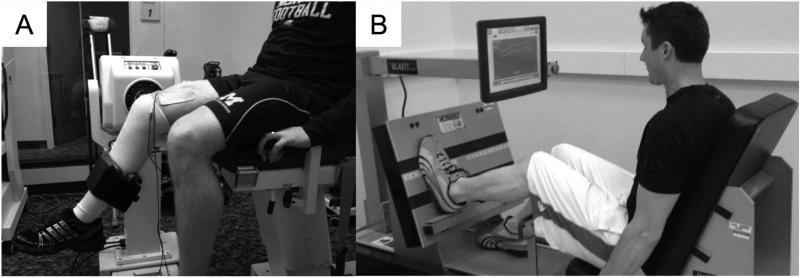
Methods: Thirty-six individuals post-injury were placed into four treatment groups (N&E, NMES and eccentrics; E-only, eccentrics only; N-only, NMES-only; and STND, standard of care) and ten healthy controls participated. N&E and N-only received the NMES protocol 2× per week for the first 6 weeks post-reconstruction. N&E and E-only received the eccentric exercise protocol 2× per week beginning 6 weeks post-reconstruction. Quadriceps activation was assessed via the superimposed burst technique and quantified via the central activation ratio. Quadriceps strength was assessed via maximal voluntary isomeric contractions (Nm/kg). Data was gathered on three occasions: pre-operative, 12-weeks-post-surgery and at return-to-play.
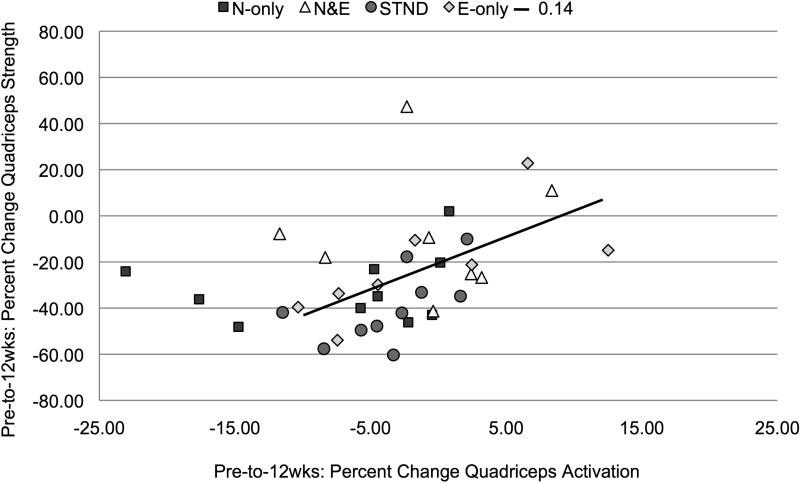
Results: No differences in pre-operative measures existed (P>0.05). E-only recovered quadriceps activation better than N-only or STND (P<0.05). N&E and E-only recovered strength better than N-only or the STND (P<0.05) and had strength values that were similar to healthy at return-to-play (P>0.05).
Conclusion: Eccentric exercise was capable of restoring levels of quadriceps activation and strength that were similar to those of healthy adults and better than NMES alone.
Level of evidence: Level 3, Parallel longitudinal study.
Keywords: ACL; Eccentric; Electrostimulation; Rehabilitation; Strength training.
Copyright © 2014 Elsevier B.V. All rights reserved.
Figures
References
-
- Palmieri-Smith RM, Thomas AC, Wojtys EM. Maximizing quadriceps strength after ACL reconstruction. Clin Sports Med. 2008;27(3):405–24. - PubMed
-
- Keays SL, Bullock-Saxton J, Newcombe P, Keays AC. The relationship between knee strength and functional stability before and after anterior cruciate ligament reconstruction. J Orthop Res. 2003;21:231–7. - PubMed
-
- Hurley MV, Jones DW, Wilson D, Newham DJ. Rehabilitation of quadriceps inhibition due to isolated rupture of the anterior cruciate ligament. Journal of Orthopaedic Rheumatology. 1992;5:145–54.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
