

Review
doi: 10.1016/j.ihj.2015.02.024.
Epub 2015 Mar 12.
How to perform transeptal puncture
Affiliations
- PMID: 25820057
- PMCID: PMC4382550
- DOI: 10.1016/j.ihj.2015.02.024
Item in Clipboard
Review
How to perform transeptal puncture
Indian Heart J.
2015 Jan-Feb.
No abstract available
Figures

a: Mullins sheath with dilator. b: Transeptal needles: The needle on the left is the Brockenbrough needle. The one in the middle is BRK needle from St Jude Medical while the needle on the right is the BRK1 needle.

AP fluoroscopic view with a Mullins sheath and Brockenbrough needle in the SVC. Pigtail catheter is placed in the aorta with the loop of the pigtail resting in the non-coronary cusp.

Brockenbrough needle inserted into the Mullins sheath with the needle flange pointing at 3 o' clock position.
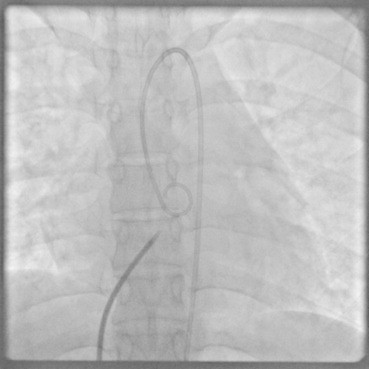
AP fluoroscopic view with the Mullins sheath and Brockenbrough needle now at the level of the aortic valve.
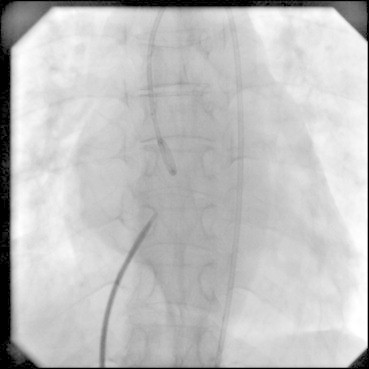
AP fluoroscopic view with the Mullins sheath and Brockenbrough needle positioned at the expected area of the fossa ovalis.

RAO projection with the Mullins sheath and Brockenbrough needle at the expected area of fossa ovalis. Note that the tip of the needle looks away from the operator.
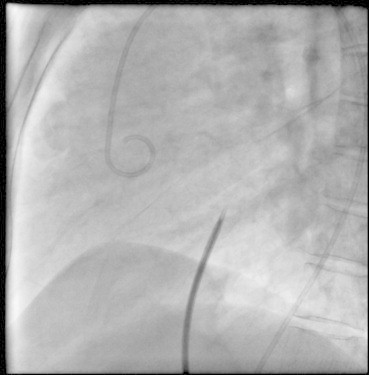
Lateral projection at the same position as in Figs. 5 and 6. The needle looks posteriorly towards the spine.
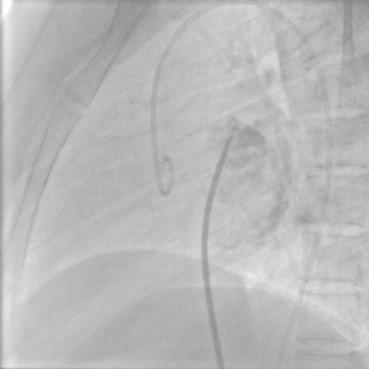
Radiographic contrast injection in the left atrium through the Mullins sheath.
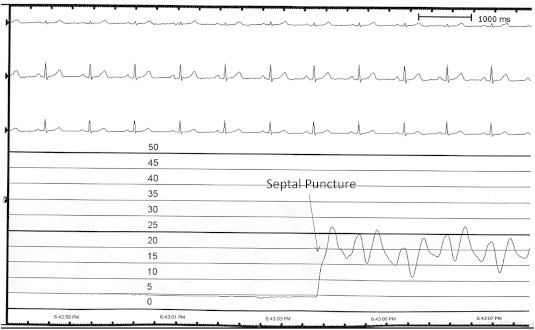
Hemodynamic trace obtained from the Mullins sheath at the fossa ovalis. The pressure recording is at 25 mm paper speed and on a 0–50 mmHg scale with each line representing 5 mmHg. The patient is in sinus rhythm. When the Mullins sheath reaches the fossa ovalis the pressure trace becomes a straight line as it abuts the septum. Once the septal puncture is performed the pressure trace and waveform of the left atrium is seen.

LAO fluoroscopic view with the needle in the same position as in Figs. 5–7. Note the slight overlap of the Brockenbrough needle with the pigtail catheter in the aorta.

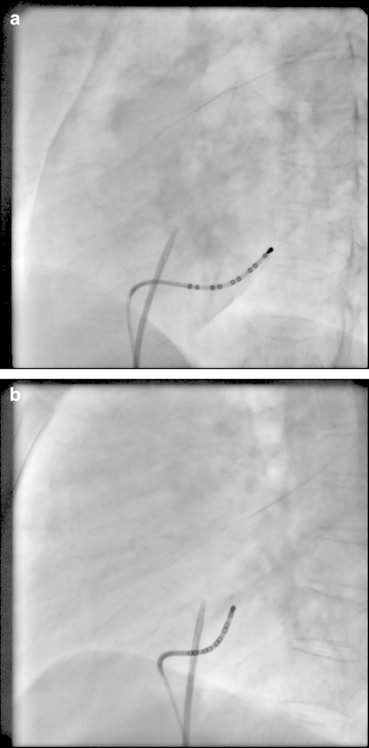
a and b, AP and RAO fluoroscopic projection with a decapolar catheter positioned in the coronary sinus and the Mullins sheath with Brockenbrough needle at the fossa ovalis. Note that the needle is posterior to the os of the coronary sinus in the RAO view.
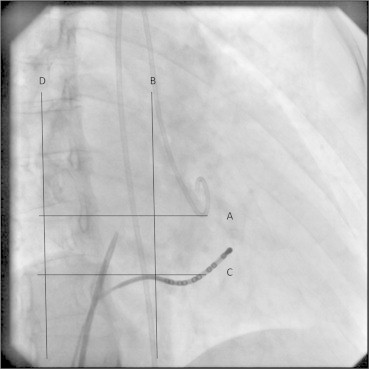
RAO projection in a patient who underwent concomitant mitral valvuloplasty and ablation of a left free wall pathway. Pigtail catheter in the aorta, decapolar catheter in the coronary sinus and Brocekenbrough needle at fossa ovalis. The needle lies approximately a centimeter below the aortic valve (line A) and posterior to both the aorta and the coronary sinus os (line B), which mark the anterior boundary of the interatrial septum. The puncture needle should not dip below coronary sinus os which also marks the anteroinferior margin of the interatrial septum (line C). The posterior margin of the left atrium is visible on the RAO projection (line D) though this overlaps with the pulmonary vein antrum and the right atrium. Septal puncture is best performed in the center of this “box” that is so formed. Entry into the left ventricle (LV) is most easily achieved if the entry is made in between lines B and D. The closer the needle is to line B, the puncture becomes more anterior and closer to the mitral annulus. This may impede easy LV entry; in difficult cases, a retro loop along the posterior wall of LA may facilitate LV entry. A high and anterior puncture risks entry into the aorta which may be catastrophic. A very posterior puncture is associated with the risk of pericardial tamponade; in some cases although the needle may enter the left atrium, it may have “stitched” the posterior walls of the right atrium and left atrium.
a and b, LAO and lateral fluoroscopic projections with the needle in the same position as Fig. 9.
Similar articles
-
Eco-X Ray Fusion for Transseptal Puncture.Rev Esp Cardiol (Engl Ed). 2015 Aug;68(8):714. doi: 10.1016/j.rec.2014.09.024. Epub 2015 Jan 28. Rev Esp Cardiol (Engl Ed). 2015. PMID: 25649971 No abstract available.
-
Guidelines on the management of valvular heart disease (version 2012).Eur Heart J. 2012 Oct;33(19):2451-96. doi: 10.1093/eurheartj/ehs109. Epub 2012 Aug 24. Eur Heart J. 2012. PMID: 22922415 No abstract available.
-
Novel robotic catheter remote control system: feasibility and safety of transseptal puncture and endocardial catheter navigation.J Cardiovasc Electrophysiol. 2006 Oct;17(10):1102-5. doi: 10.1111/j.1540-8167.2006.00556.x. Epub 2006 Jul 18. J Cardiovasc Electrophysiol. 2006. PMID: 16879628
-
Echocardiographic-Fluoroscopic Fusion Imaging in Transseptal Puncture: A New Technology for an Old Procedure.J Am Soc Echocardiogr. 2017 Sep;30(9):886-895. doi: 10.1016/j.echo.2017.05.001. Epub 2017 Jun 7. J Am Soc Echocardiogr. 2017. PMID: 28601385 Review.
-
Angio-Guidewire-Ultrasound (AGU) Guidance for Femoral Access in Procedures Requiring Large Sheaths.J Invasive Cardiol. 2019 Feb;31(2):E37-E39. doi: 10.25270/jic/18.00173. J Invasive Cardiol. 2019. PMID: 30700629 Review.
Cited by
-
Unconventional combination of left atrial appendage device occlusion in patients with atrial fibrillation who needed concomitant catheter interventions for underlying structural heart disease.Indian Heart J. 2020 Sep-Oct;72(5):369-375. doi: 10.1016/j.ihj.2020.07.019. Epub 2020 Jul 28. Indian Heart J. 2020. PMID: 33189196 Free PMC article.
-
Implementation of a zero fluoroscopic workflow using a simplified intracardiac echocardiography guided method for catheter ablation of atrial fibrillation, including repeat procedures.BMC Cardiovasc Disord. 2021 Aug 26;21(1):407. doi: 10.1186/s12872-021-02219-8. BMC Cardiovasc Disord. 2021. PMID: 34433424 Free PMC article.
-
An anthropomorphic phantom for atrial transseptal puncture simulation training.3D Print Med. 2024 Oct 30;10(1):34. doi: 10.1186/s41205-024-00241-y. 3D Print Med. 2024. PMID: 39472399 Free PMC article.
-
Venoplasty of a chronic venous occlusion with 'diathermy' for cardiac device lead placement.Indian Pacing Electrophysiol J. 2019 Jan-Feb;19(1):27-29. doi: 10.1016/j.ipej.2018.10.002. Epub 2018 Oct 25. Indian Pacing Electrophysiol J. 2019. PMID: 30367925 Free PMC article.
-
Transseptal Puncture: Devices, Techniques, and Considerations for Specific Interventions.Curr Cardiol Rep. 2019 May 7;21(6):52. doi: 10.1007/s11886-019-1136-6. Curr Cardiol Rep. 2019. PMID: 31065869 Review.
References
-
- Ross J., Jr., Braunwald E., Morrow A.G. Left heart catheterization by the transeptal route: a description of the technique and its applications. Circulation. 1960;22:927–934.
-
- Brockenbrough E.C., Braunwald E., Ross J., Jr. Transseptal left heart catheterization. A review of 450 studies and description of an improved technic. Circulation. 1962;25:15–21. - PubMed
-
- Mullins C.E. Transseptal left heart catheterization: experience with a new technique in 520 pediatric and adult patients. Pediatr Cardiol. 1983;4:239–245. - PubMed
-
- Hung J.S. Atrial septal puncture technique in percutaneous transvenous mitral commissurotomy : mitral valvuloplasty using the lnoue balloon catheter technique. Cathet Cardiovasc Diagn. 1992;26:275–284. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
