Elastofibroma dorsi: a histochemical and immunohistochemical study
- PMID: 25820560
- PMCID: PMC4378214
- DOI: 10.4081/ejh.2015.2459
Elastofibroma dorsi: a histochemical and immunohistochemical study
Abstract
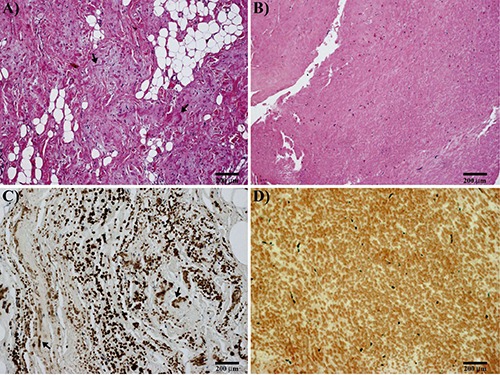
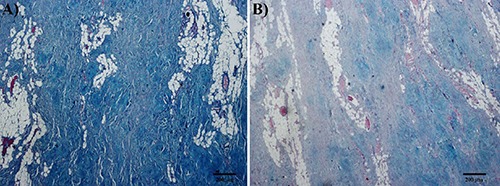
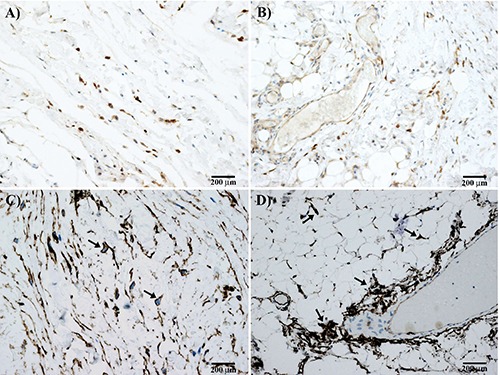
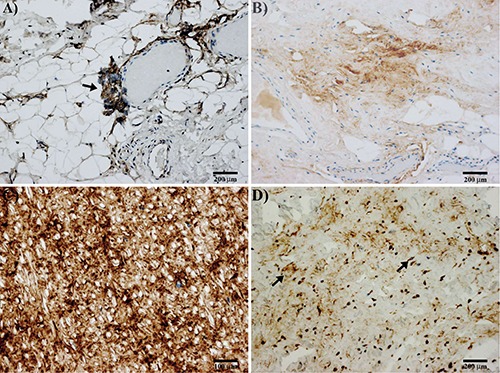
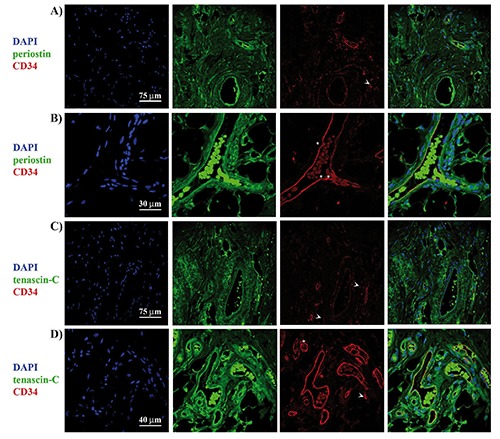
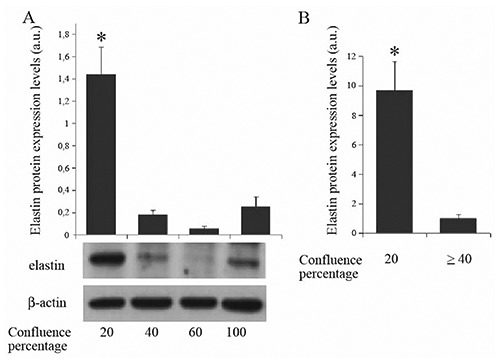
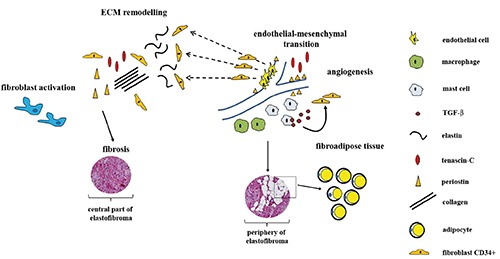
Elastofibroma dorsi (ED) is considered a member of a heterogeneous group of benign fibrous (fibroblastic or myofibroblastic) soft-tissue tumors, frequently localized in the periscapular region in middle aged or older individuals. However, the pathogenesis of ED is still unclear and many authors believe that ED results from a reactive hyperproliferation of fibroblastic tissue, while others suggest that it may be a consequence of a mechanical friction. In our study, we examined 11 cases of ED using histochemical and immunohistochemical methods, in order to extend the knowledge about extracellular matrix composition and histopathogenesis of ED. From the results it appeared that stroma and interspersed spindle cells of ED were positive for both periostin and tenascin-C. Mast cells tryptase-positive were also abundant throughout the lesion. The perivascular distribution of periostin and tenascin-C, associated with the CD34 positivity, suggest that endothelial-mesenchymal transition events can account for neovascularization and production of fibroelastic tissue characteristic of elastofibroma. Our data obtained in endothelial cells cultures demonstrated that elastin production is higher when the status of confluence of the cells is low. So, we can assume that such a phenomenon is a characteristic of mesenchymal/endothelial cells CD34 positive, in which elastin production results to be inversely proportional to the vascular differentiation of cellular elements. In the light of these considerations, we think that a cancerous nature of ED is unlikely. Overall, our study report, for the first time, a detailed description of extracellular matrix composition in ED, suggesting that a mechanical strain-dependent reactivation of periostin and tenascin-C expression, as well as of elastin deposition, could be responsible for development of ED.
Conflict of interest statement
Conflicts of interest: the authors declare no conflicts of interest.
Figures
References
-
- Hisaoka M, Nishio JN. Elastofibroma, p. 53-4. Fletcher DM, Bridge JA, Hogendoorn CW, Mertens F.(eds.), WHO classification of tumors of soft tissue and bone. International Agency for research on cancer, Lyon: 2013.
-
- Naylor MF, Nascimento AG, Sherrick AD, McLeod RA. Elastofibroma dorsi: radiologic findings in 12 patients. AJR Am J Roentgenol 1996;167:683-7. - PubMed
-
- Schick S, Zembsch A, Gahleitner A, Wanderbaldinger P, Amann G, Breitenseher M, et al. Atypical appearance of elastofibroma dorsi on MRI: case reports and review of the literature. J Comput Assist Tomogr 2000;24:288-92. - PubMed
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Miscellaneous