

Effects of Electroacupuncture with Dominant Frequency at SP 6 and ST 36 Based on Meridian Theory on Pain-Depression Dyad in Rats
- PMID: 25821498
- PMCID: PMC4364048
- DOI: 10.1155/2015/732845
Effects of Electroacupuncture with Dominant Frequency at SP 6 and ST 36 Based on Meridian Theory on Pain-Depression Dyad in Rats
Abstract
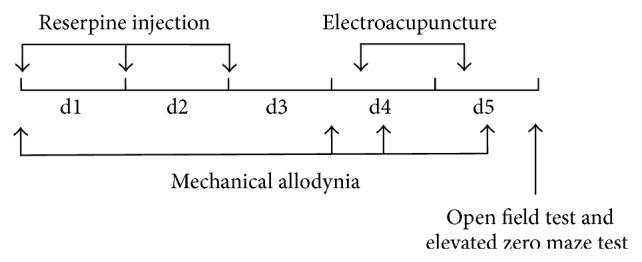
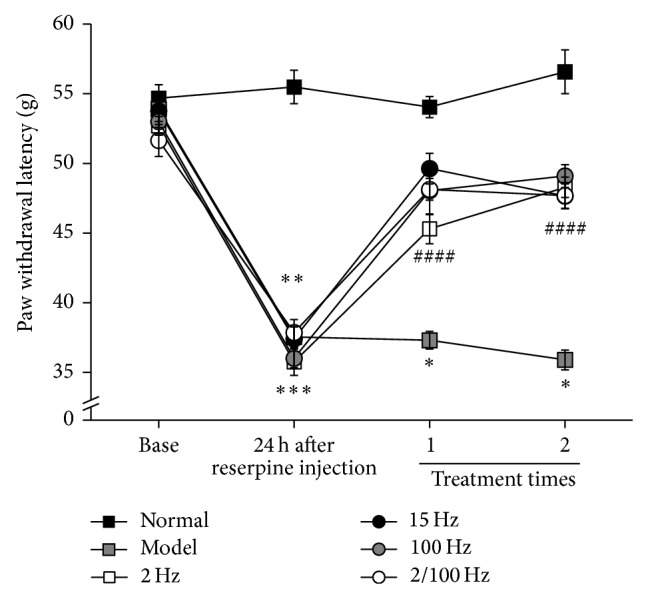
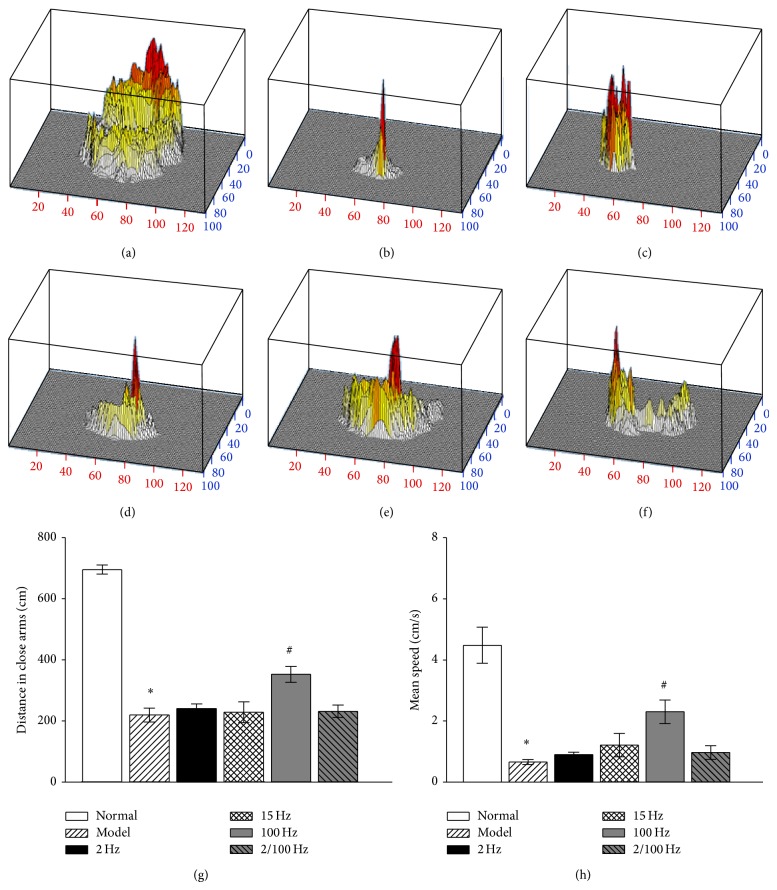
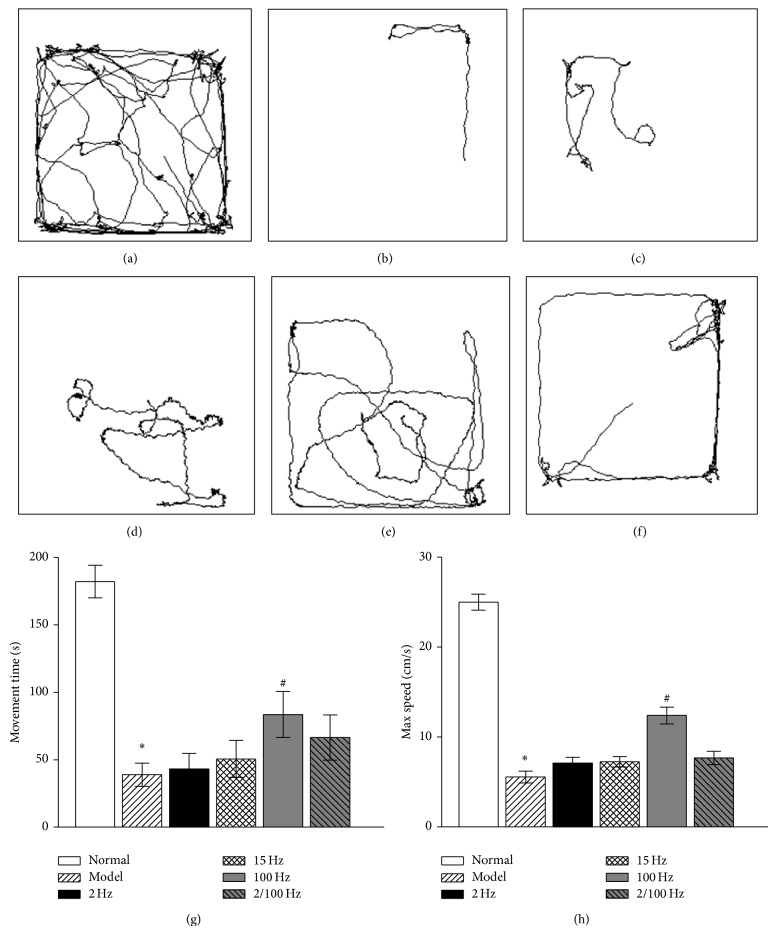
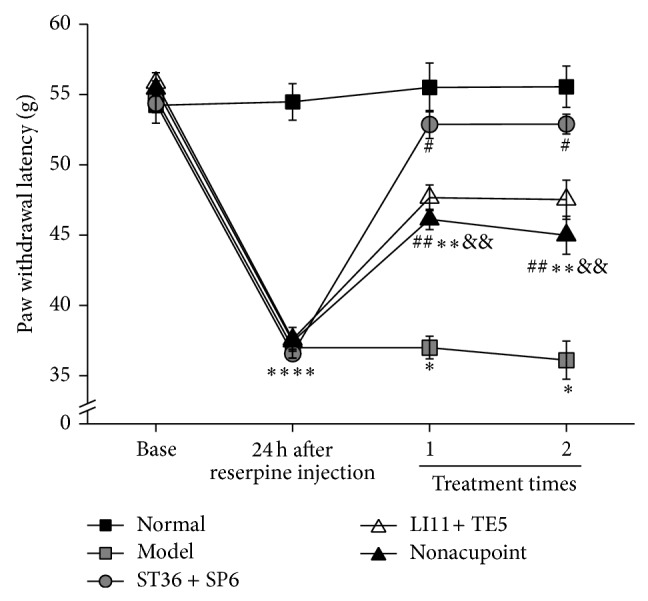
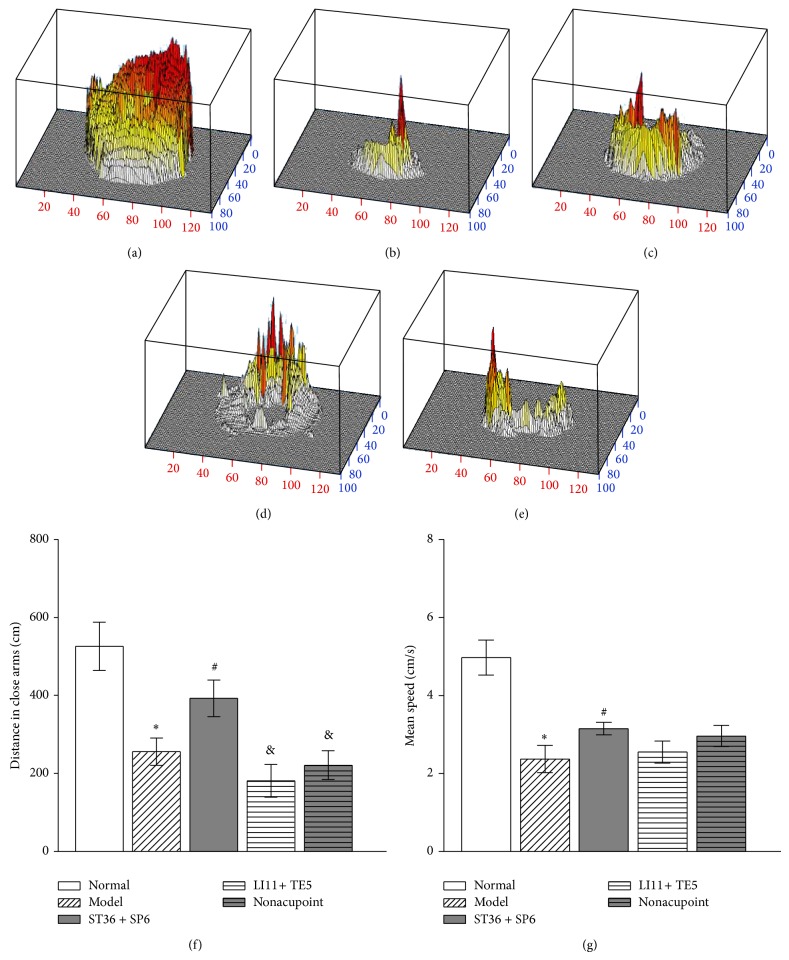
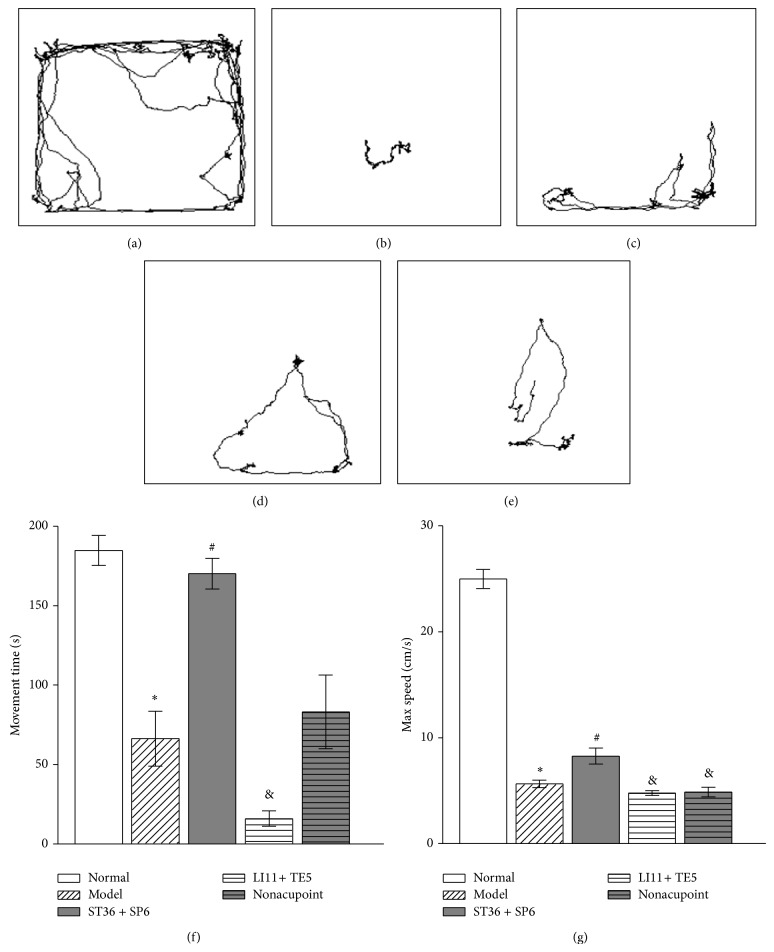
Epidemic investigations reveal an intimate interrelationship between pain and depression. The effect of electroacupuncture (EA) on pain or depression has been demonstrated individually, but its effect on pain-depression dyad is unknown. Our study aimed to screen a dominant EA frequency on pain-depression dyad and determine the validity of acupoint selection based on meridian theory. The pain-depression dyad rat model was induced by reserpine and treated using EA with different frequencies at identical acupoints to extract a dominant frequency and then administrated dominant-frequency EA at different acupoints in the above models. Paw withdrawal latency (PWL), emotional behavior of elevated zero maze (EZM) test, and open field (OF) test were conducted. We found that 100 Hz EA at Zusanli (ST 36) and Sanyinjiao (SP 6) (classical acupoints for spleen-deficiency syndrome) were the most effective in improving PWL, travelling distance in the EZM, and maximum velocity in OF compared to EA with other frequencies; ST 36 and SP 6 were proved more effective than other acupoints beyond the meridian theory and nonacupoints under the same administration of EA. Therefore, we concluded that 100 Hz is the dominant frequency for treating the pain-depression dyad with EA, and acupoints on spleen and stomach meridians are preferable choices.
Figures
Similar articles
-
[Relationship between efficacy of electroacupuncture and electroacupuncture stimulation of different acupoints and different tissue layers of acupoint area in hypotension plus bradycardia rats].Zhen Ci Yan Jiu. 2010 Dec;35(6):422-8. Zhen Ci Yan Jiu. 2010. PMID: 21375015 Chinese.
-
[Prescription analysis of electroacupuncture for simple obesity based on complex network technique].Zhongguo Zhen Jiu. 2018 Mar 12;38(3):331-6. doi: 10.13703/j.0255-2930.2018.03.028. Zhongguo Zhen Jiu. 2018. PMID: 29701055 Chinese.
-
[Time-effect relationship and molecular mechanism of electroacupuncture for repair of gastric mucosal lesion].Zhongguo Zhen Jiu. 2018 Jul 12;38(7):747-52. doi: 10.13703/j.0255-2930.2018.07.018. Zhongguo Zhen Jiu. 2018. PMID: 30014670 Chinese.
-
[Clinical research and the effect mechanism on premature ovarian failure treated with acupuncture in recent 20 years].Zhongguo Zhen Jiu. 2018 May 12;38(5):5653-70. doi: 10.13703/j.0255-2930.2018.05.031. Zhongguo Zhen Jiu. 2018. PMID: 29797923 Review. Chinese.
-
[Discussion on rules of acupoint selection for vascular dementia].Zhongguo Zhen Jiu. 2017 Jul 12;37(7):785-790. doi: 10.13703/j.0255-2930.2017.07.026. Zhongguo Zhen Jiu. 2017. PMID: 29231557 Review. Chinese.
Cited by
-
Effect of Electroacupuncture at Different Acupoints on the Expression of NMDA Receptors in ACC and Colon in IBS Rats.Evid Based Complement Alternat Med. 2019 Feb 3;2019:4213928. doi: 10.1155/2019/4213928. eCollection 2019. Evid Based Complement Alternat Med. 2019. PMID: 30854008 Free PMC article.
-
Beneficial effect of electroacupuncture on the distribution of foreign substances in the brain of rats developing depression-like behavior.IBRO Neurosci Rep. 2023 Mar 28;14:398-406. doi: 10.1016/j.ibneur.2023.03.014. eCollection 2023 Jun. IBRO Neurosci Rep. 2023. PMID: 37388496 Free PMC article.
-
Pain aversion and anxiety-like behavior occur at different times during the course of chronic inflammatory pain in rats.J Pain Res. 2017 Nov 6;10:2585-2593. doi: 10.2147/JPR.S139679. eCollection 2017. J Pain Res. 2017. PMID: 29158690 Free PMC article.
-
Mechanisms of acupuncture in treating depression: a review.Chin Med. 2025 Mar 3;20(1):29. doi: 10.1186/s13020-025-01080-7. Chin Med. 2025. PMID: 40033393 Free PMC article. Review.
-
Auricular acupuncture plays a neuroprotective role in 6-hydroxydopamine-induced Parkinson's disease in rats.J Tradit Complement Med. 2024 May 28;15(2):128-139. doi: 10.1016/j.jtcme.2024.05.008. eCollection 2025 Mar. J Tradit Complement Med. 2024. PMID: 40060148 Free PMC article.
References
-
- Tunks E. R., Crook J., Weir R. Epidemiology of chronic pain with psychological comorbidity: prevalence, risk, course, and prognosis. Canadian Journal of Psychiatry. 2008;53(4):224–234. - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
