

Detection of Rheumatoid Arthritis-Interstitial Lung Disease Is Enhanced by Serum Biomarkers
- PMID: 25822095
- PMCID: PMC4476561
- DOI: 10.1164/rccm.201411-1950OC
Detection of Rheumatoid Arthritis-Interstitial Lung Disease Is Enhanced by Serum Biomarkers
Abstract
Rationale: Interstitial lung disease (ILD), a leading cause of morbidity and mortality in rheumatoid arthritis (RA), is highly prevalent, yet RA-ILD is underrecognized.
Objectives: To identify clinical risk factors, autoantibodies, and biomarkers associated with the presence of RA-ILD.
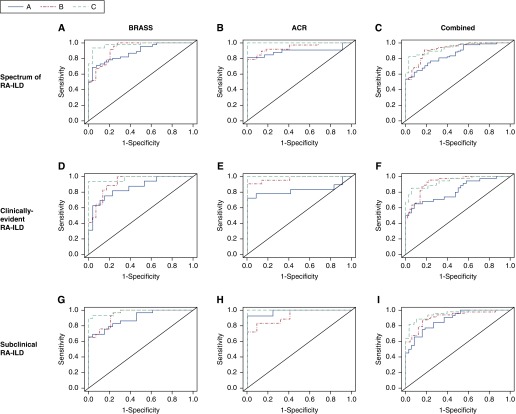
Methods: Subjects enrolled in Brigham and Women's Hospital Rheumatoid Arthritis Sequential Study (BRASS) and American College of Rheumatology (ACR) cohorts were evaluated for ILD. Regression models were used to assess the association between variables of interest and RA-ILD. Receiver operating characteristic curves were generated in BRASS to determine if a combination of clinical risk factors and autoantibodies can identify RA-ILD and if the addition of investigational biomarkers is informative. This combinatorial signature was subsequently tested in ACR.
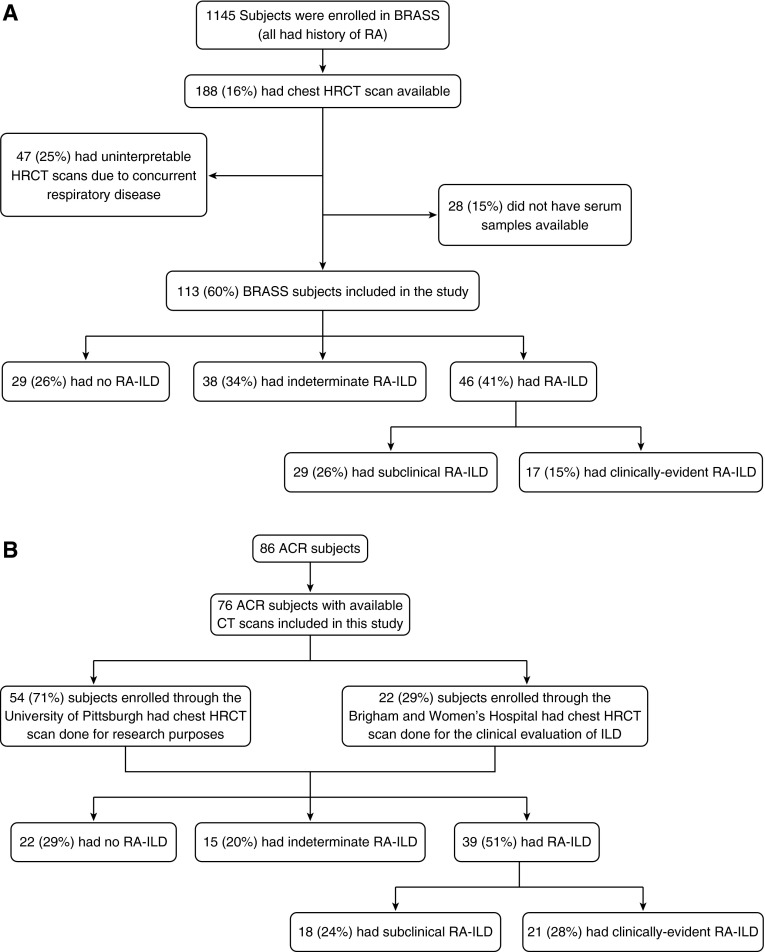
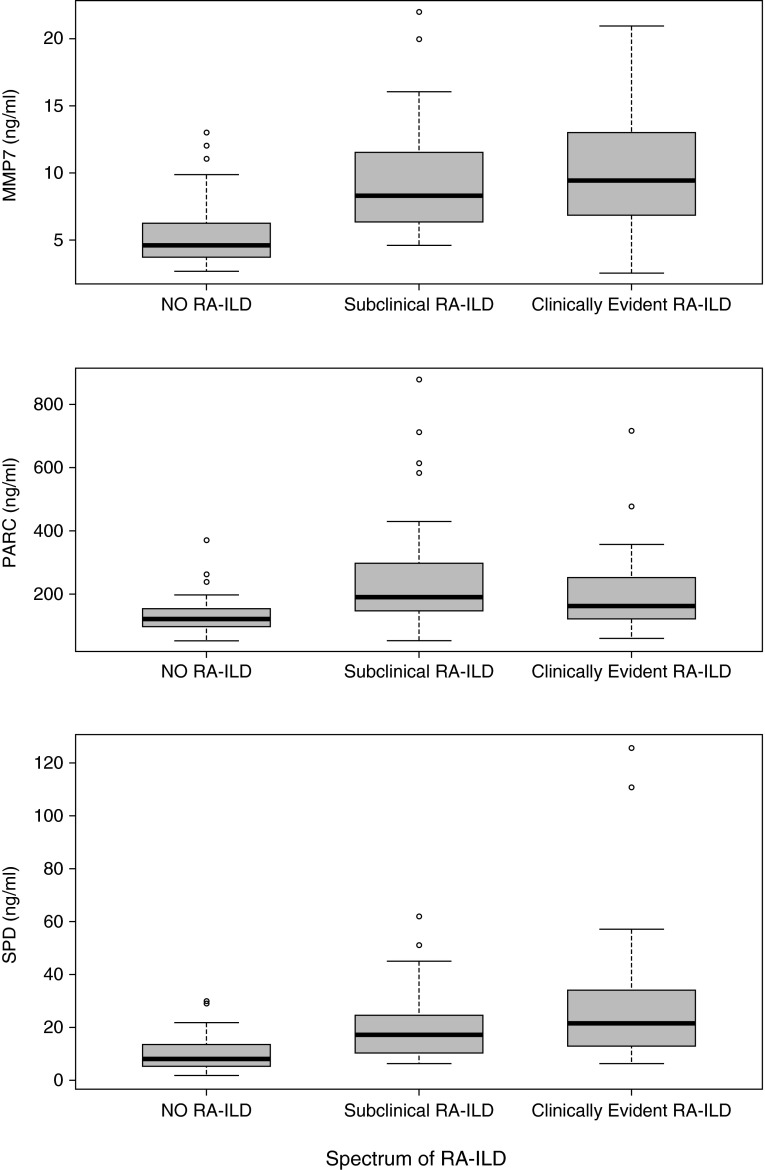
Measurements and main results: A total of 113 BRASS subjects with clinically indicated chest computed tomography scans (41% with a spectrum of clinically evident and subclinical RA-ILD) and 76 ACR subjects with research or clinical scans (51% with a spectrum of RA-ILD) were selected. A combination of age, sex, smoking, rheumatoid factor, and anticyclic citrullinated peptide antibodies was strongly associated with RA-ILD (areas under the curve, 0.88 for BRASS and 0.89 for ACR). Importantly, a combinatorial signature including matrix metalloproteinase 7, pulmonary and activation-regulated chemokine, and surfactant protein D significantly increased the areas under the curve to 0.97 (P = 0.002, BRASS) and 1.00 (P = 0.016, ACR). Similar trends were seen for both clinically evident and subclinical RA-ILD.
Conclusions: Clinical risk factors and autoantibodies are strongly associated with the presence of clinically evident and subclinical RA-ILD on computed tomography scan in two independent RA cohorts. A biomarker signature composed of matrix metalloproteinase 7, pulmonary and activation-regulated chemokine, and surfactant protein D significantly strengthens this association. These findings may facilitate identification of RA-ILD at an earlier stage, potentially leading to decreased morbidity and mortality.
Keywords: biomarkers; interstitial lung disease; rheumatoid arthritis; risk prediction; subclinical.
Figures
Comment in
-
Molecular Phenotyping. A Guide to Improving Detection of Interstitial Lung Disease in Patients with Rheumatoid Arthritis.Am J Respir Crit Care Med. 2015 Jun 15;191(12):1349-50. doi: 10.1164/rccm.201504-0751ED. Am J Respir Crit Care Med. 2015. PMID: 26075419 No abstract available.
References
-
- Scott DL, Wolfe F, Huizinga TW. Rheumatoid arthritis. Lancet. 2010;376:1094–1108. - PubMed
-
- Sacks JJ, Luo YH, Helmick CG. Prevalence of specific types of arthritis and other rheumatic conditions in the ambulatory health care system in the United States, 2001-2005. Arthritis Care Res (Hoboken) 2010;62:460–464. - PubMed
-
- Saag KG, Teng GG, Patkar NM, Anuntiyo J, Finney C, Curtis JR, Paulus HE, Mudano A, Pisu M, Elkins-Melton M, et al. American College of Rheumatology. American College of Rheumatology 2008 recommendations for the use of nonbiologic and biologic disease-modifying antirheumatic drugs in rheumatoid arthritis. Arthritis Rheum. 2008;59:762–784. - PubMed
-
- Young A, Koduri G, Batley M, Kulinskaya E, Gough A, Norton S, Dixey J Early Rheumatoid Arthritis Study (ERAS) group. Mortality in rheumatoid arthritis: increased in the early course of disease, in ischaemic heart disease and in pulmonary fibrosis. Rheumatology (Oxford) 2007;46:350–357. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
