

Protocol for Reducing Time to Antibiotics in Pediatric Patients Presenting to an Emergency Department With Fever and Neutropenia: Efficacy and Barriers
- PMID: 25822237
- PMCID: PMC4584166
- DOI: 10.1097/PEC.0000000000000362
Protocol for Reducing Time to Antibiotics in Pediatric Patients Presenting to an Emergency Department With Fever and Neutropenia: Efficacy and Barriers
Abstract
Objectives: Patients with febrile neutropenia are at high risk of morbidity and mortality from infectious causes. Decreasing time to antibiotic (TTA) administration is associated with improved patient outcomes. We sought to reduce TTA for children presenting to the emergency department with fever and neutropenia.
Methods: In a prospective cohort study with historical comparison, TTA administration was evaluated in patients with neutropenia presenting to the Children's of Alabama Emergency Department. A protocol was established to reduce delays in antibiotic administration and increase the percentage of patients who receive treatment within 60 minutes of presentation. One hundred pre-protocol patient visits between August 2010 and December 2011 were evaluated and 153 post-protocol visits were evaluated between August 2012 and September 2013. We reviewed individual cases to determine barriers to rapid antibiotic administration.
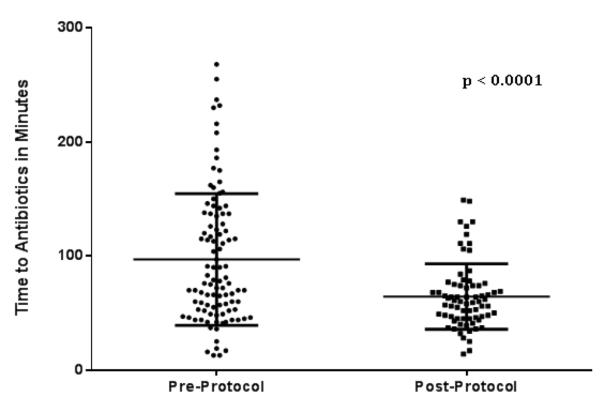
Results: Antibiotics were administered in 96.9 ± 57.8 minutes in the pre-protocol patient group, and only 35% of patients received antibiotics within 60 minutes of presentation and 70% received antibiotics within 120 minutes. After implementation of the protocol, TTA for neutropenic patients was decreased to 64.3 ± 28.4 minutes (P < 0.0001) with 51.4% receiving antibiotics within 60 minutes and 93.2% within 120 minutes.
Conclusions: Implementing a standard approach to patients at risk for neutropenia decreased TTA. There are numerous challenges in providing timely antibiotics to children with febrile neutropenia. Identified delays included venous access (time to effect of topical anesthetics, and difficulty obtaining access), physicians waiting on laboratory results, and antibiotic availability.
Figures




References
-
- Freifeld AG, Bow EJ, Sepkowitz KA, et al. Clinical practice guideline for the use of antimicrobial agents in neutropenic patients with cancer: 2010 update by the infectious diseases society of america. Clin Infect Dis. 2011 Feb 15;52(4):e56–93. - PubMed
-
- Gonzalez-Barca E, Fernandez-Sevilla A, Carratala J, et al. Prognostic factors influencing mortality in cancer patients with neutropenia and bacteremia. Eur J Clin Microbiol Infect Dis. 1999 Aug;18(8):539–544. - PubMed
-
- Elting LS, Rubenstein EB, Rolston KV, Bodey GP. Outcomes of bacteremia in patients with cancer and neutropenia: observations from two decades of epidemiological and clinical trials. Clin Infect Dis. 1997 Aug;25(2):247–259. - PubMed
-
- Santolaya ME, Alvarez AM, Aviles CL, et al. Admission clinical and laboratory factors associated with death in children with cancer during a febrile neutropenic episode. Pediatr Infect Dis J. 2007 Sep;26(9):794–798. - PubMed
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
