

Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas, 2008-2013: results from population-based surveillance
- PMID: 25822249
- PMCID: PMC4378850
- DOI: 10.1371/journal.pone.0120452
Declining incidence of candidemia and the shifting epidemiology of Candida resistance in two US metropolitan areas, 2008-2013: results from population-based surveillance
Abstract
Background: Recent reports have demonstrated a decline in bacterial bloodstream infections (BSIs) following adherence to central line insertion practices; however, declines have been less evident for BSIs due to Candida species.
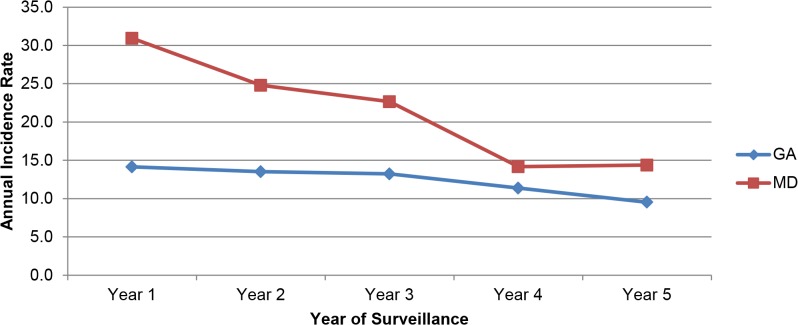
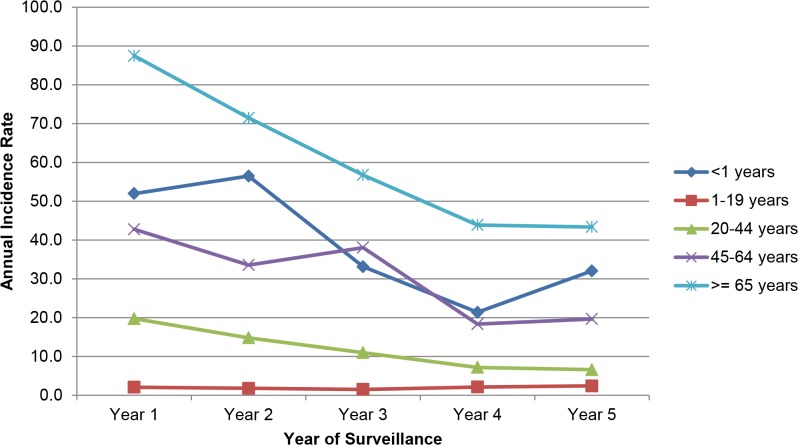
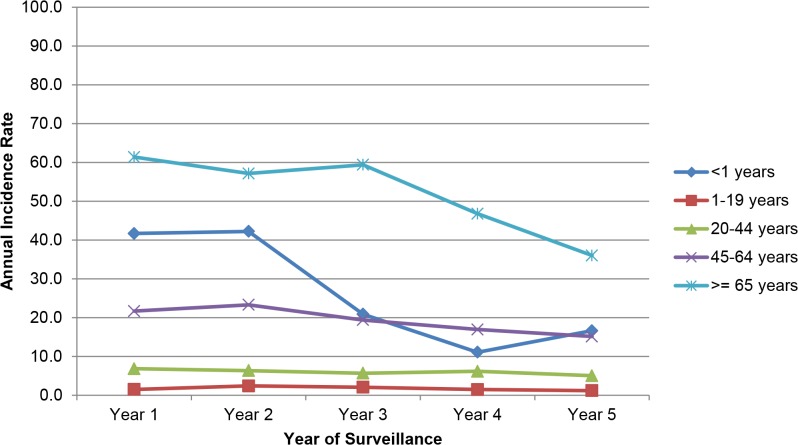
Methods: We conducted active, population-based laboratory surveillance for candidemia in metropolitan Atlanta, GA and Baltimore, MD over a 5-year period. We calculated annual candidemia incidence and antifungal drug resistance rates.
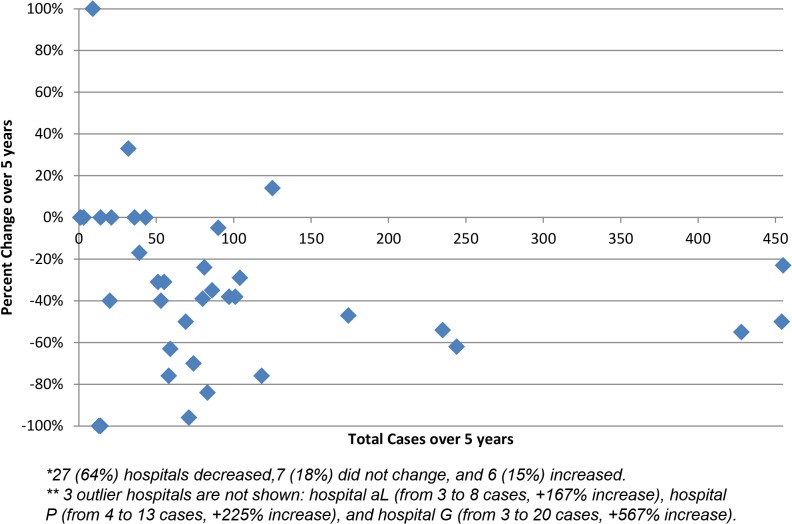
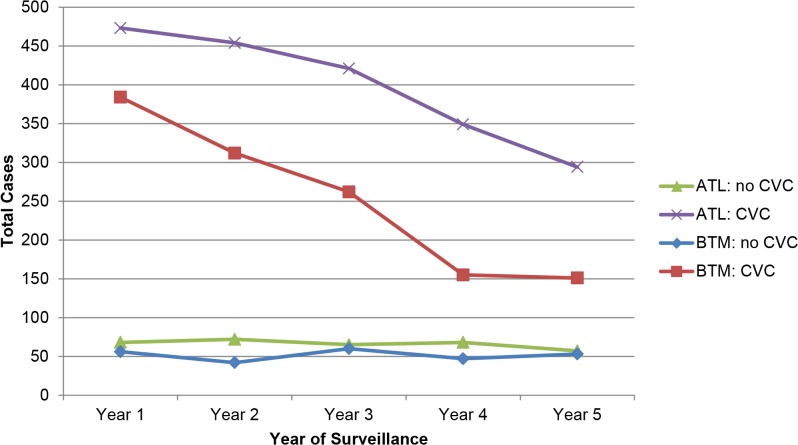
Results: We identified 3,848 candidemia cases from 2008-2013. Compared with 2008, candidemia incidence per 100,000 person-years decreased significantly by 2013 in both locations (GA: 14.1 to 9.5, p<0.001; MD: 30.9 to 14.4, p<0.001). A total of 3,255 cases (85%) had a central venous catheter (CVC) in place within 2 days before the BSI culture date. In both locations, the number of CVC-associated cases declined (GA: 473 to 294; MD: 384 to 151). Candida albicans (CA, 36%) and Candida glabrata (CG, 27%) were the most common species recovered. In both locations, the proportion of cases with fluconazole resistance decreased (GA: 8.0% to 7.1%, -10%; MD: 6.6% to 4.9%, -25%), while the proportion of cases with an isolate resistant to an echinocandin increased (GA: 1.2% to 2.9%, +147%; MD: 2.0% to 3.5%, +77%). Most (74%) echinocandin-resistant isolates were CG; 17 (<1%) isolates were resistant to both drug categories (multidrug resistant [MDR], 16/17 were CG). The proportion of CG cases with MDR Candida increased from 1.8% to 2.6%.
Conclusions: We observed a significant decline in the incidence of candidemia over a five-year period, and increases in echinocandin-resistant and MDR Candida. Efforts to strengthen infection control practices may be preventing candidemia among high-risk patients. Further surveillance for resistant Candida is warranted.
Conflict of interest statement
Figures
References
-
- US Department of Health and Human Services (USDHHS). National Action Plan to Reduce Healthcare-Associated Infections. Washington, DC. 2010. Available at http://www.hhs.gov/ash/initiatives/hai/actionplan/index.html. Accessed December 2, 2013.
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
