

Multidimensional clinical phenotyping of an adult cystic fibrosis patient population
- PMID: 25822311
- PMCID: PMC4378917
- DOI: 10.1371/journal.pone.0122705
Multidimensional clinical phenotyping of an adult cystic fibrosis patient population
Abstract
Background: Cystic Fibrosis (CF) is a multi-systemic disease resulting from mutations in the Cystic Fibrosis Transmembrane Regulator (CFTR) gene and has major manifestations in the sino-pulmonary, and gastro-intestinal tracts. Clinical phenotypes were generated using 26 common clinical variables to generate classes that overlapped quantiles of lung function and were based on multiple aspects of CF systemic disease.
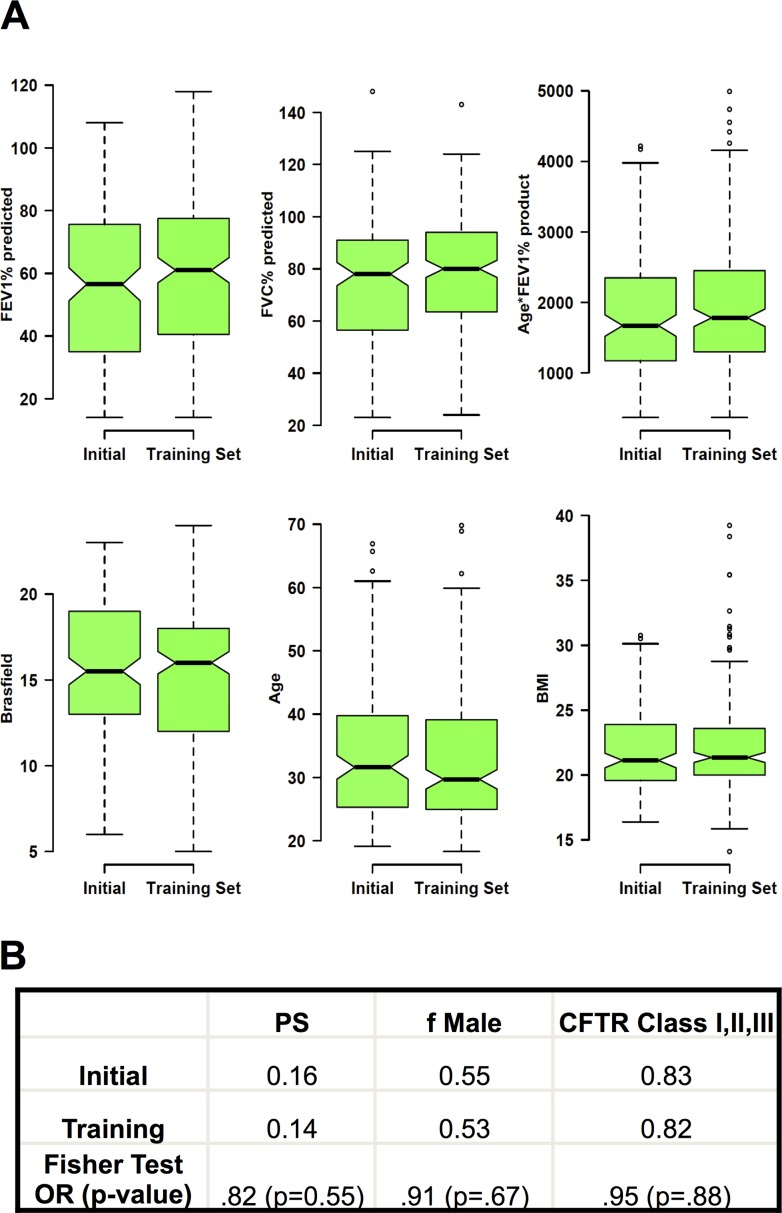
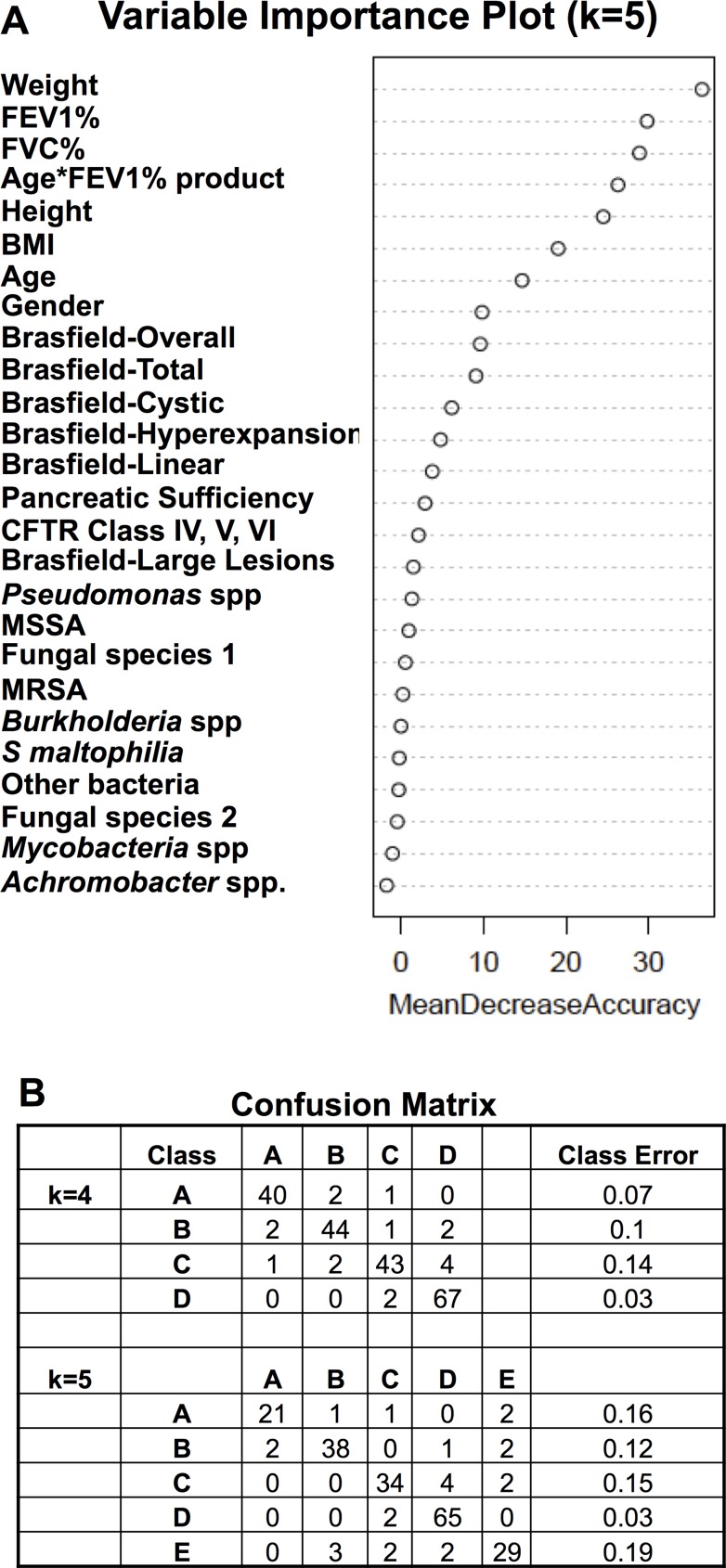
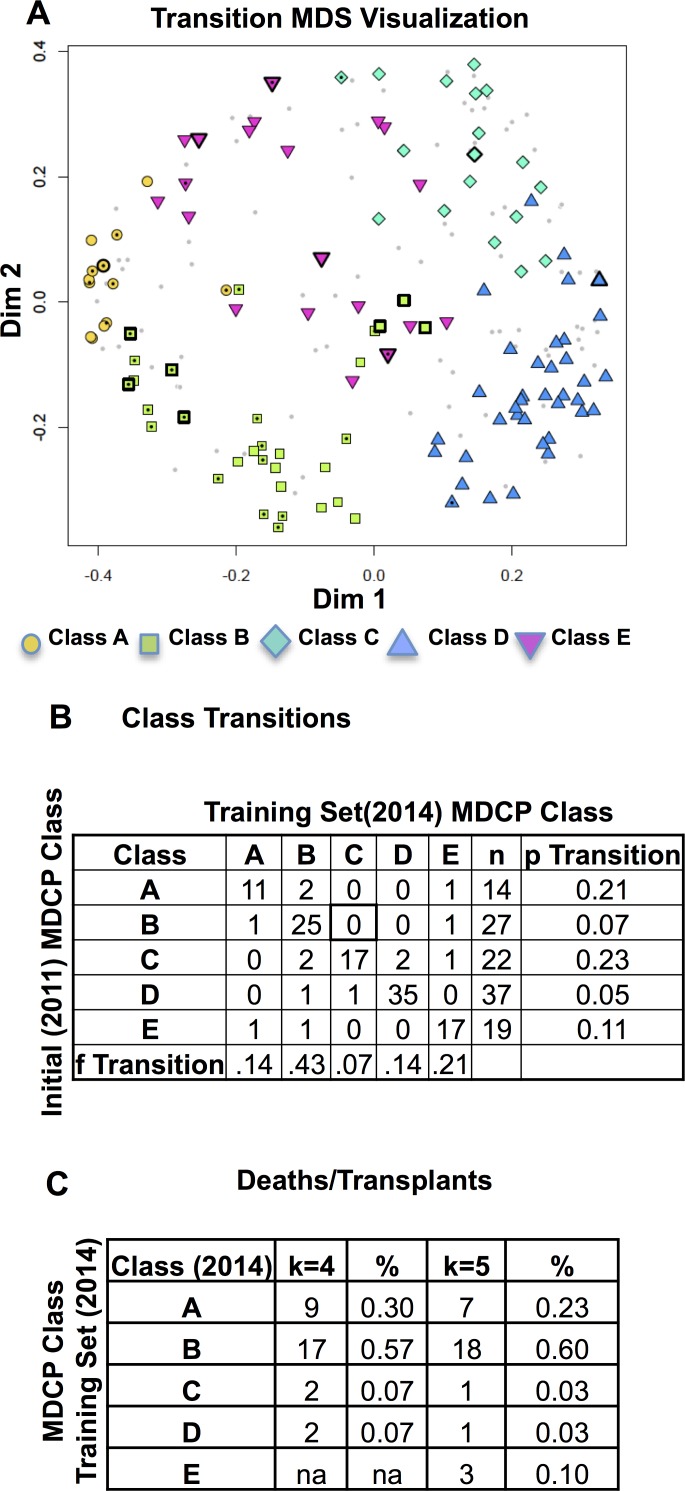
Methods: The variables included age, gender, CFTR mutations, FEV1% predicted, FVC% predicted, height, weight, Brasfield chest xray score, pancreatic sufficiency status and clinical microbiology results. Complete datasets were compiled on 211 subjects. Phenotypes were identified using a proximity matrix generated by the unsupervised Random Forests algorithm and subsequent clustering by the Partitioning around Medoids (PAM) algorithm. The final phenotypic classes were then characterized and compared to a similar dataset obtained three years earlier.
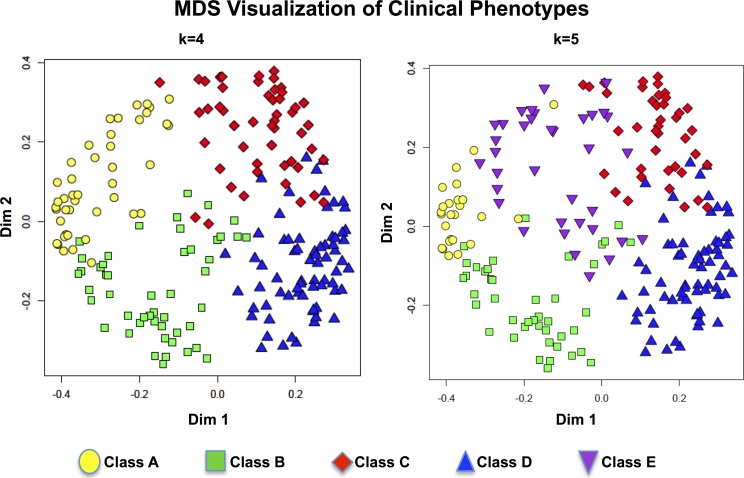
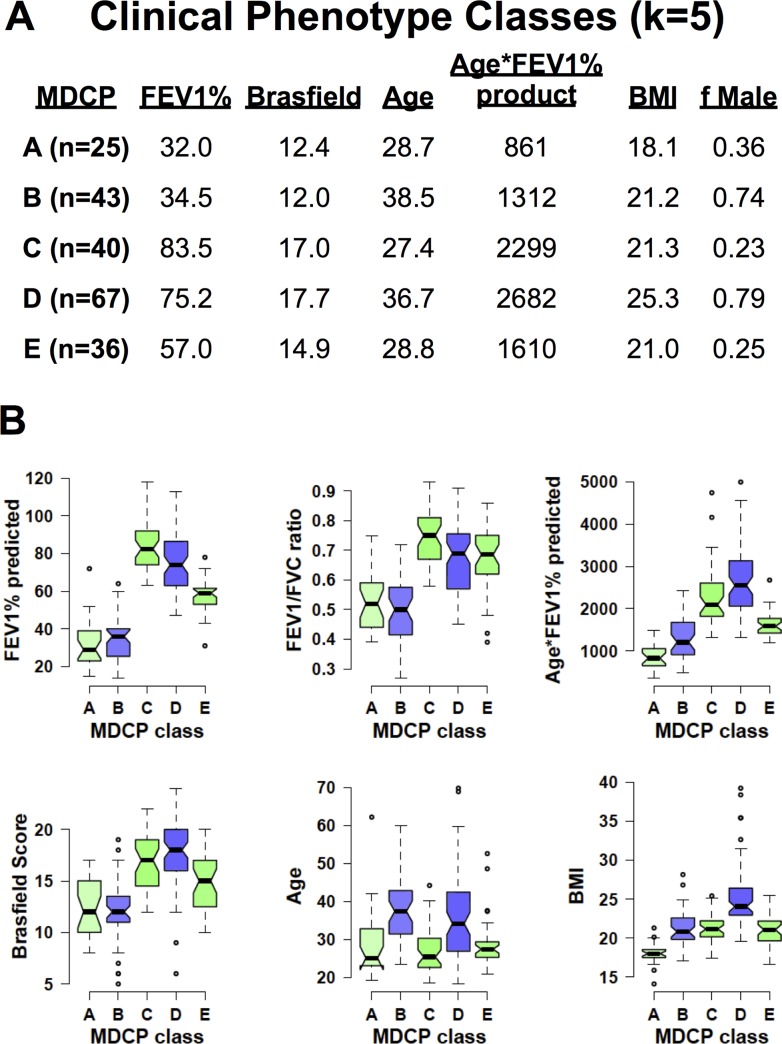
Findings: Clinical phenotypes were identified using a clustering strategy that generated four and five phenotypes. Each strategy identified 1) a low lung health scores phenotype, 2) a younger, well-nourished, male-dominated class, 3) various high lung health score phenotypes that varied in terms of age, gender and nutritional status. This multidimensional clinical phenotyping strategy identified classes with expected microbiology results and low risk clinical phenotypes with pancreatic sufficiency.
Interpretation: This study demonstrated regional adult CF clinical phenotypes using non-parametric, continuous, ordinal and categorical data with a minimal amount of subjective data to identify clinically relevant phenotypes. These studies identified the relative stability of the phenotypes, demonstrated specific phenotypes consistent with published findings and identified others needing further study.
Conflict of interest statement
Figures
Similar articles
-
Multi-dimensional clinical phenotyping of a national cohort of adult cystic fibrosis patients.J Cyst Fibros. 2021 Jan;20(1):91-96. doi: 10.1016/j.jcf.2020.08.010. Epub 2020 Sep 15. J Cyst Fibros. 2021. PMID: 32948498
-
CFTR genotype and clinical outcomes of adult patients carried as cystic fibrosis disease.Gene. 2014 May 1;540(2):183-90. doi: 10.1016/j.gene.2014.02.040. Epub 2014 Feb 26. Gene. 2014. PMID: 24583165
-
Clinical implications of cystic fibrosis transmembrane conductance regulator mutations.Clin Chest Med. 1998 Sep;19(3):443-58, v. doi: 10.1016/s0272-5231(05)70092-7. Clin Chest Med. 1998. PMID: 9759548 Review.
-
[Italian Cystic Fibrosis Registry (ICFR). Report 2015-2016].Epidemiol Prev. 2019 Jul-Aug;43(4S1):1-36. doi: 10.19191/EP19.4.S1.067. Epidemiol Prev. 2019. PMID: 31370382 Italian.
-
[Cystic fibrosis transmembrane conductance regulator (CFTR) gene: mutations and clinical phenotypes].Ugeskr Laeger. 2003 Feb 24;165(9):912-6. Ugeskr Laeger. 2003. PMID: 12661515 Review. Danish.
Cited by
-
A machine learning approach using partitioning around medoids clustering and random forest classification to model groups of farms in regard to production parameters and bulk tank milk antibody status of two major internal parasites in dairy cows.PLoS One. 2022 Jul 11;17(7):e0271413. doi: 10.1371/journal.pone.0271413. eCollection 2022. PLoS One. 2022. PMID: 35816512 Free PMC article.
-
Beyond Antagonism: The Interaction Between Candida Species and Pseudomonas aeruginosa.J Fungi (Basel). 2019 Apr 19;5(2):34. doi: 10.3390/jof5020034. J Fungi (Basel). 2019. PMID: 31010211 Free PMC article. Review.
-
Neutrophilic proteolysis in the cystic fibrosis lung correlates with a pathogenic microbiome.Microbiome. 2019 Feb 13;7(1):23. doi: 10.1186/s40168-019-0636-3. Microbiome. 2019. PMID: 30760325 Free PMC article.
-
Personalized Web-Based Cognitive Rehabilitation Treatments for Patients with Traumatic Brain Injury: Cluster Analysis.JMIR Med Inform. 2020 Oct 6;8(10):e16077. doi: 10.2196/16077. JMIR Med Inform. 2020. PMID: 33021482 Free PMC article.
-
Median regression spline modeling of longitudinal FEV1 measurements in cystic fibrosis (CF) and chronic obstructive pulmonary disease (COPD) patients.PLoS One. 2017 Dec 20;12(12):e0190061. doi: 10.1371/journal.pone.0190061. eCollection 2017. PLoS One. 2017. PMID: 29261779 Free PMC article.
References
-
- Cystic Fibrosis Foundation Patient Registry. Cystic Fibrosis Foundation, 2012.
-
- Drumm ML, Konstan MW, Schluchter MD, Handler A, Pace R, Zou F, et al. Genetic modifiers of lung disease in cystic fibrosis. N Engl J Med 2005; 353: 1443–53. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
