

Normalized lactate load is associated with development of acute kidney injury in patients who underwent cardiopulmonary bypass surgery
- PMID: 25822369
- PMCID: PMC4378943
- DOI: 10.1371/journal.pone.0120466
Normalized lactate load is associated with development of acute kidney injury in patients who underwent cardiopulmonary bypass surgery
Abstract
Background and objective: Cardiac surgery associated acute kidney injury is a major postoperative complication and has long been associated with adverse outcomes. However, the association of lactate and AKI has not been well established. The study aimed to explore the association of normalized lactate load with AKI in patients undergoing cardiac surgery.
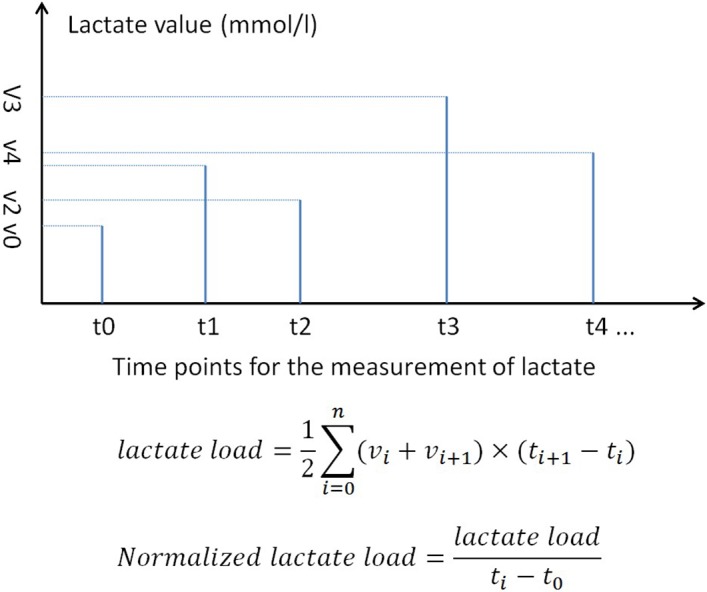
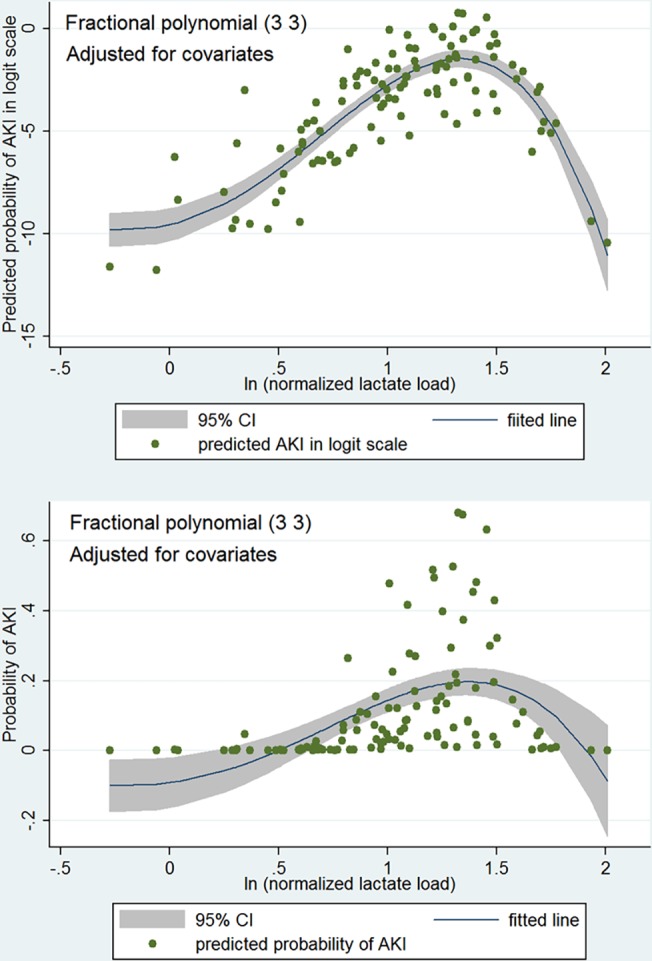
Methods: This was a prospective observational cohort study conducted in a 47-bed ICU of a tertiary academic teaching hospital from July 2012 to January 2014. All patients undergoing cardiopulmonary bypass surgery were included. Normalized lactate load (L) was calculated by the equation: [Formula: see text], where ti was time point for lactate measurement and vi was the value of lactate. L was transformed by natural log (Lln) to improve its normality. Logistic regression model was fitted by using stepwise method. Scale of Lln was examined by using fractional polynomial approach and potential interaction terms were explored.
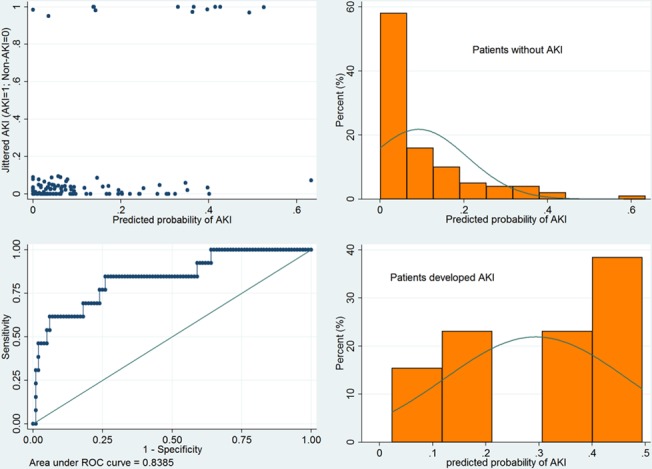
Results: A total of 117 patients were included during study period, including 17 AKI patients and 100 non-AKI patients. In univariate analysis Lln was significantly higher in AKI as compared with non-AKI group (1.43±0.38 vs 1.01±0.45, p = 0.0005). After stepwise selection of covariates, the main effect logistic model contained variables of Lln (odds ratio: 11.1, 95% CI: 1.22-101.6), gender, age, baseline serum creatinine and fluid balance on day 0. Although the two-term fractional polynomial model was the best-fitted model, it was not significantly different from the linear model (Deviance difference = 6.09, p = 0.107). There was no significant interaction term between Lln and other variables in the main effect model.
Conclusions: Our study demonstrates that Lln is independently associated with postoperative AKI in patients undergoing CPB. There is no significant interaction with early postoperative fluid balance.
Conflict of interest statement
Figures
References
-
- Uchino S, Kellum JA, Bellomo R, Doig GS, Morimatsu H, et al. (2005) Acute renal failure in critically ill patients: a multinational, multicenter study. JAMA 294: 813–818. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
