

Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
- PMID: 25823771
- PMCID: PMC4517513
- DOI: 10.1038/ajg.2015.65
Forty-Year Analysis of Colonoscopic Surveillance Program for Neoplasia in Ulcerative Colitis: An Updated Overview
Abstract
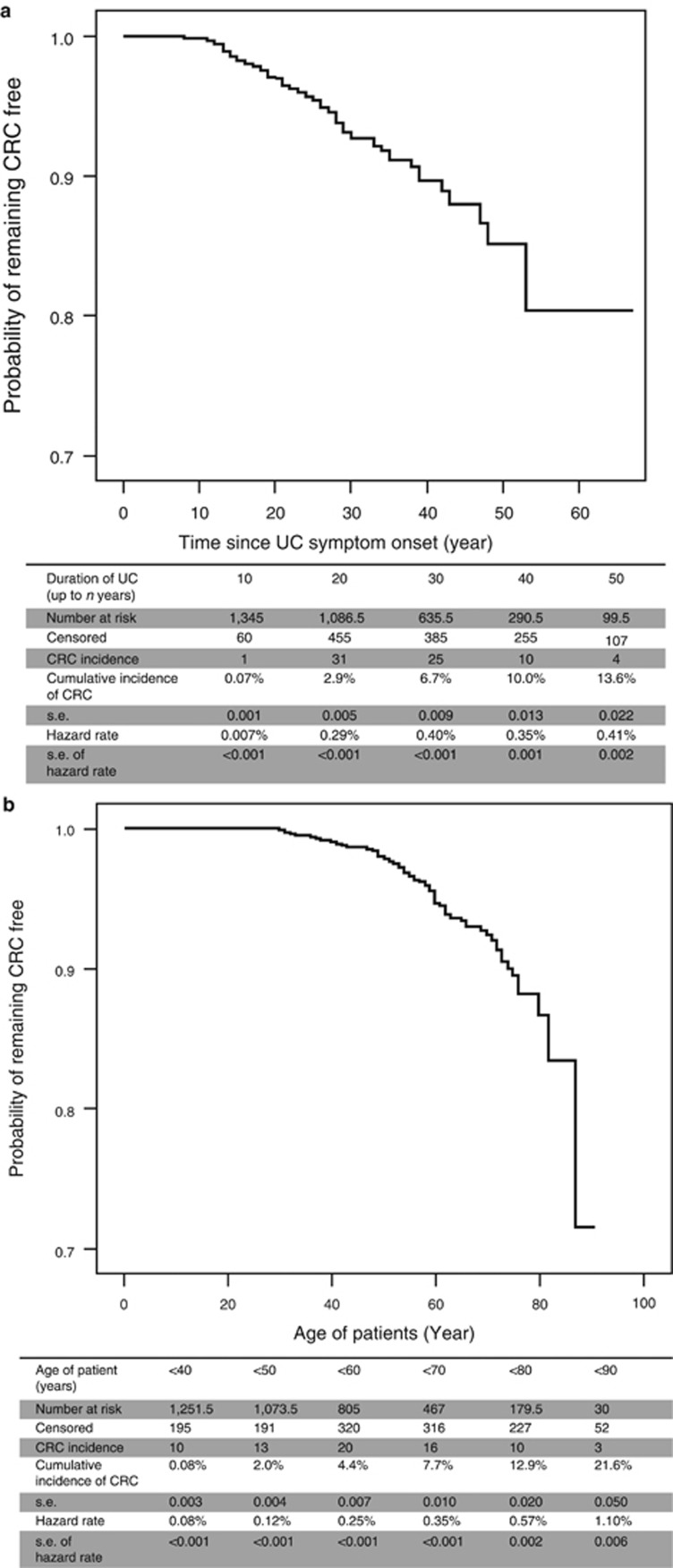
Objectives: This study provides an overview of the largest and longest-running colonoscopic surveillance program for colorectal cancer (CRC) in patients with long-standing ulcerative colitis (UC).
Methods: Data were obtained from medical records, endoscopy, and histology reports. Primary end points were defined as death, colectomy, withdrawal from surveillance, or censor date (1 January 2013).
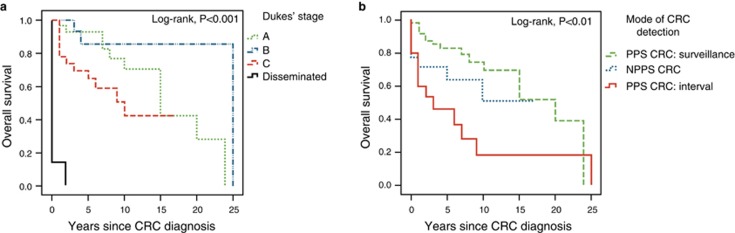
Results: A total of 1,375 UC patients were followed up for 15,234 patient-years (median, 11 years per patient). CRC was detected in 72 patients (incidence rate (IR), 4.7 per 1,000 patient-years). Time-trend analysis revealed that although there was significant decrease in incidence of colectomy performed for dysplasia (linear regression, R=-0.43; P=0.007), IR of advanced CRC and interval CRC have steadily decreased over past four decades (Pearson's correlation, -0.99; P=0.01 for both trends). The IR of early CRC has increased 2.5-fold in the current decade compared with past decade (χ(2), P=0.045); however, its 10-year survival rate was high (79.6%). The IR of dysplasia has similarly increased (χ(2), P=0.01), potentially attributable to the recent use of chromoendoscopy that was twice more effective at detecting dysplasia compared with white-light endoscopy (χ(2), P<0.001). CRCs were frequently accompanied by synchronous CRC or spatially distinct dysplasia (37.5%). Finally, the risk of CRC was not significantly different between "indefinite" or low-grade dysplasia (log-rank, P=0.78).
Conclusions: Colonoscopic surveillance may have a significant role in reducing the risk of advanced and interval CRC while allowing more patients to retain their colon for longer. Given the ongoing risk of early CRC, patients with any grade of dysplasia who are managed endoscopically should be monitored closely with advanced techniques.
Figures





Comment in
-
Miles to Go on the SCENIC Route: Should Chromoendoscopy Become the Standard of Care in IBD Surveillance?Am J Gastroenterol. 2015 Jul;110(7):1035-7. doi: 10.1038/ajg.2015.179. Am J Gastroenterol. 2015. PMID: 26148262
References
-
- Rutter MD, Saunders BP, Wilkinson KH, et al. Thirty-year analysis of a colonoscopic surveillance program for neoplasia in ulcerative colitis. Gastroenterology. 2006;130:1030–1038. - PubMed
-
- Jess T, Simonsen J, Jørgensen KT, et al. Decreasing risk of colorectal cancer in patients with inflammatory bowel disease over 30 years Gastroenterology 2012143375–381.e1; quiz e13–4.. - PubMed
-
- Söderlund S, Brandt L, Lapidus A, et al. Decreasing time-trends of colorectal cancer in a large cohort of patients with inflammatory bowel disease Gastroenterology 20091361561–1567.quiz 1818–9.. - PubMed
-
- Marion JF, Waye JD, Present DH, et al. Chromoendoscopy-targeted biopsies are superior to standard colonoscopic surveillance for detecting dysplasia in inflammatory bowel disease patients: a prospective endoscopic trial. Am J Gastroenterol. 2008;103:2342–2349. - PubMed
-
- Kiesslich R, Fritsch J, Holtmann M, et al. Methylene blue-aided chromoendoscopy for the detection of intraepithelial neoplasia and colon cancer in ulcerative colitis. Gastroenterology. 2003;124:880–888. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
