

Predictive monitoring for sepsis and necrotizing enterocolitis to prevent shock
- PMID: 25823938
- PMCID: PMC11742165
- DOI: 10.1016/j.siny.2015.03.006
Predictive monitoring for sepsis and necrotizing enterocolitis to prevent shock
Abstract
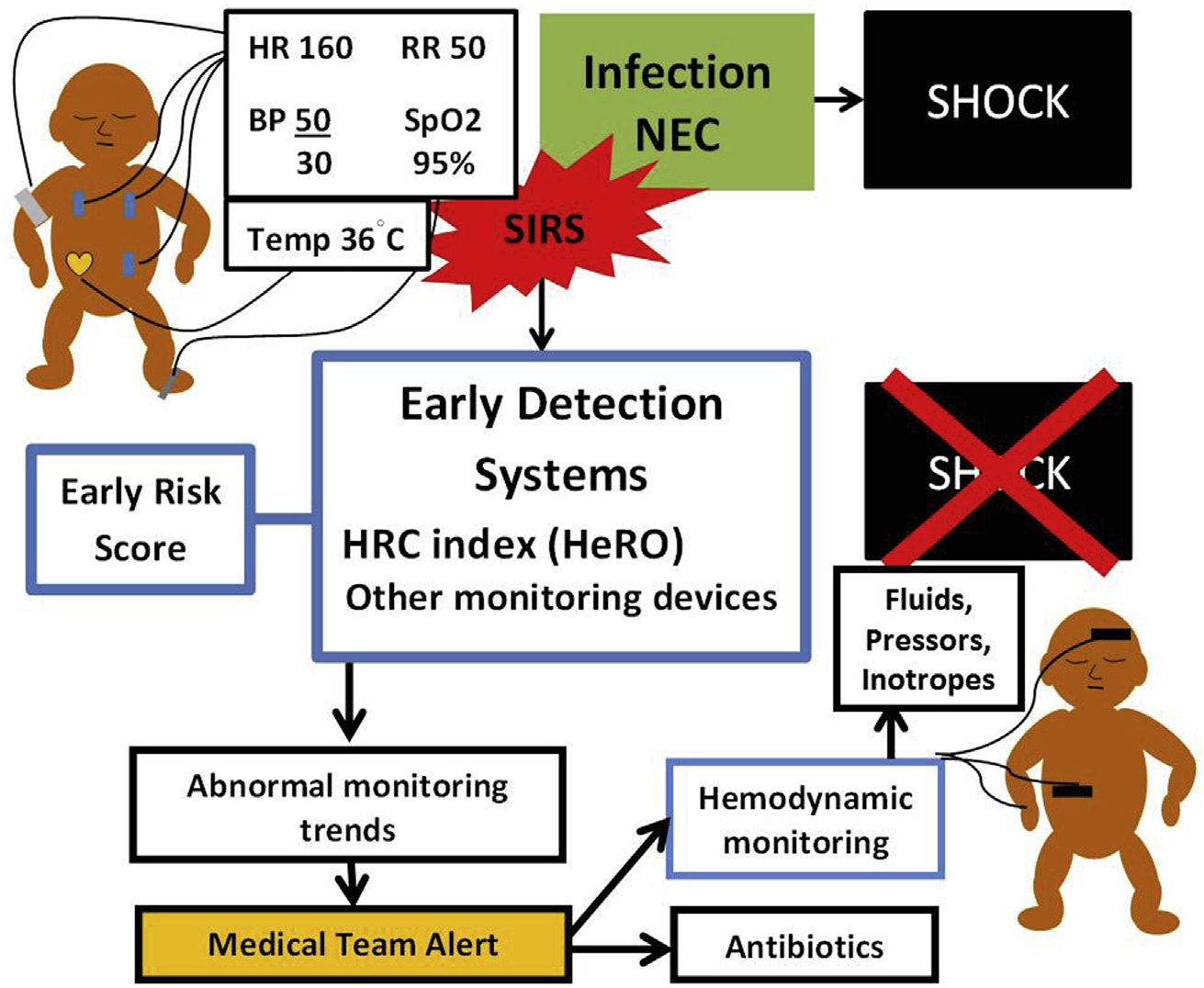
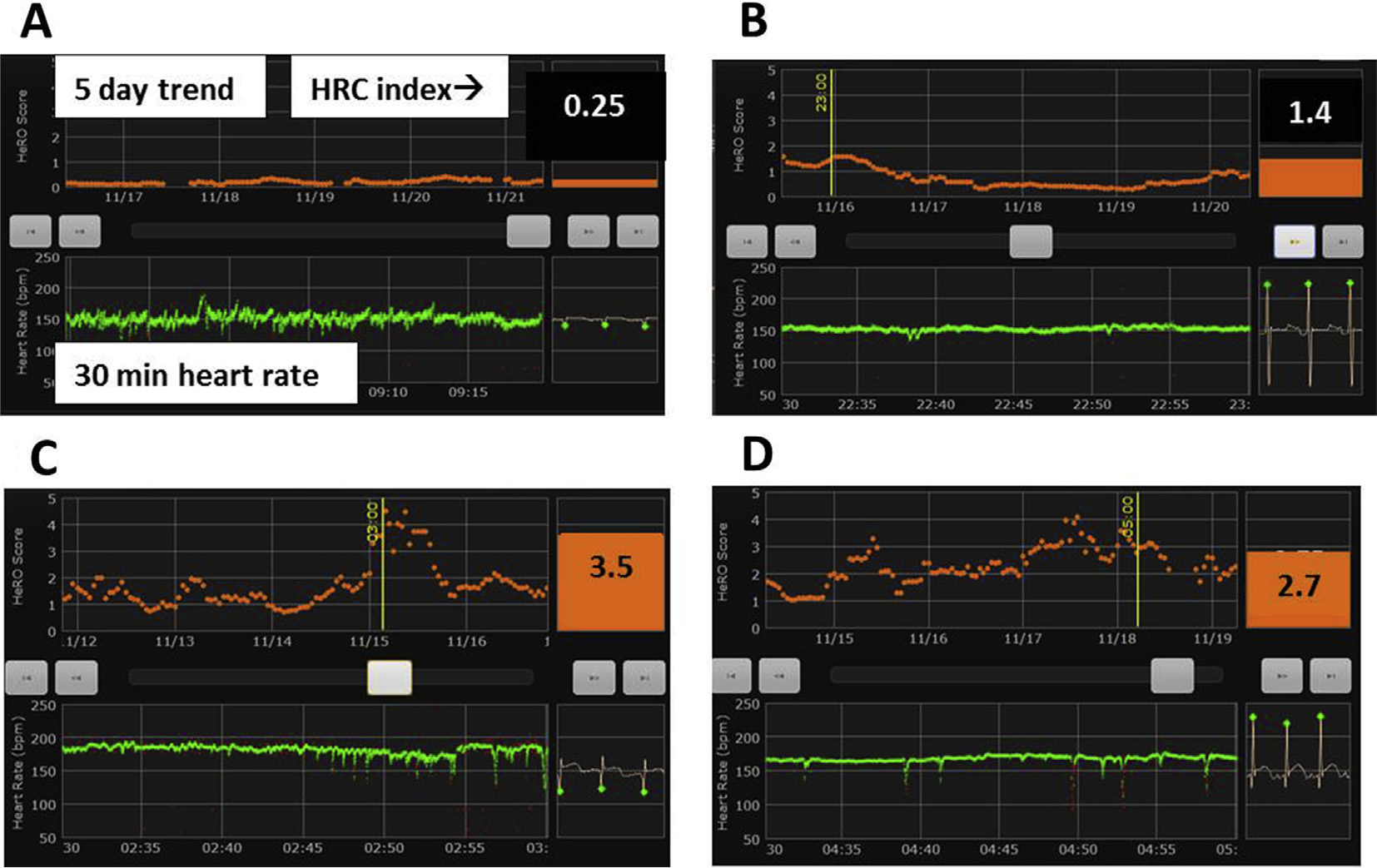
Despite vigilant clinical assessment of infants in the neonatal intensive care unit (NICU), diagnosis of sepsis and necrotizing enterocolitis often does not occur until an infant has significant hemodynamic compromise. Predictive monitoring involves analysis of vital signs and other clinical data to identify infants at highest risk and to detect early-stage illness, leading to timelier treatment and improved outcomes. The first vital-sign predictive monitoring device developed for sepsis detection in babies in the NICU is the heart rate characteristics index (HeRO) monitor, which continuously analyzes the electrocardiogram signal for low heart rate variability and transient decelerations. Use of this monitor in very low birth weight infants (<1500 g) was shown in a large multicenter randomized clinical trial to significantly reduce mortality. The purpose of this review is (1) to summarize the physiologic changes in neonatal sepsis and progression to shock, (2) to review efforts toward risk stratification for sepsis shortly after birth based on demographic and physiologic scoring systems, (3) to describe development and implementation of heart rate characteristics monitoring and other important aspects of sepsis early warning systems, and (4) to provide an overview of current research analyzing multiple vital signs and other clinical variables in an attempt to develop even more effective predictive monitoring devices and systems.
Keywords: Heart rate characteristic monitoring; Heart rate characteristics index; Necrotizing enterocolitis; Predictive monitoring; Sepsis; Shock; Systemic inflammatory response syndrome.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
Conflict of interest statement
None declared.
Figures
Similar articles
-
Vital signs and their cross-correlation in sepsis and NEC: a study of 1,065 very-low-birth-weight infants in two NICUs.Pediatr Res. 2017 Feb;81(2):315-321. doi: 10.1038/pr.2016.215. Epub 2016 Nov 3. Pediatr Res. 2017. PMID: 28001143 Free PMC article.
-
Heart rate characteristics: physiomarkers for detection of late-onset neonatal sepsis.Clin Perinatol. 2010 Sep;37(3):581-98. doi: 10.1016/j.clp.2010.06.002. Clin Perinatol. 2010. PMID: 20813272 Free PMC article. Review.
-
Predictive monitoring for early detection of sepsis in neonatal ICU patients.Curr Opin Pediatr. 2013 Apr;25(2):172-9. doi: 10.1097/MOP.0b013e32835e8fe6. Curr Opin Pediatr. 2013. PMID: 23407184 Free PMC article. Review.
-
The NICU Antibiotics and Outcomes (NANO) trial: a randomized multicenter clinical trial assessing empiric antibiotics and clinical outcomes in newborn preterm infants.Trials. 2022 May 23;23(1):428. doi: 10.1186/s13063-022-06352-3. Trials. 2022. PMID: 35606829 Free PMC article. Clinical Trial.
-
Vital signs analysis algorithm detects inflammatory response in premature infants with late onset sepsis and necrotizing enterocolitis.Early Hum Dev. 2018 Feb;117:83-89. doi: 10.1016/j.earlhumdev.2018.01.008. Epub 2018 Jan 23. Early Hum Dev. 2018. PMID: 29351876 Free PMC article.
Cited by
-
Bench to bedside - new insights into the pathogenesis of necrotizing enterocolitis.Nat Rev Gastroenterol Hepatol. 2022 Jul;19(7):468-479. doi: 10.1038/s41575-022-00594-x. Epub 2022 Mar 28. Nat Rev Gastroenterol Hepatol. 2022. PMID: 35347256 Review.
-
Enteral Feeding and Antibiotic Treatment Do Not Influence Increased Coefficient of Variation of Total Fecal Bile Acids in Necrotizing Enterocolitis.Newborn (Clarksville). 2023;2(2):128-132. doi: 10.5005/jp-journals-11002-0063. Epub 2023 May 7. Newborn (Clarksville). 2023. PMID: 37559695 Free PMC article.
-
Improving Neonatal Care with Technology.Front Pediatr. 2017 May 15;5:110. doi: 10.3389/fped.2017.00110. eCollection 2017. Front Pediatr. 2017. PMID: 28555182 Free PMC article. No abstract available.
-
Safety and efficacy of colistin and fluoroquinolone in neonatal persistent late-onset sepsis.Saudi Pharm J. 2021 Sep;29(9):1013-1020. doi: 10.1016/j.jsps.2021.07.014. Epub 2021 Jul 21. Saudi Pharm J. 2021. PMID: 34588847 Free PMC article.
-
Vital signs as physiomarkers of neonatal sepsis.Pediatr Res. 2022 Jan;91(2):273-282. doi: 10.1038/s41390-021-01709-x. Epub 2021 Sep 7. Pediatr Res. 2022. PMID: 34493832 Review.
References
-
- Goldstein B, Giroir B, Randolph A. International pediatric sepsis consensus conference: definitions for sepsis and organ dysfunction in pediatrics. Pediatr Crit Care Med 2005;6:2–8. - PubMed
-
- Hofer N, Zacharias E, Müller W, Resch B. Performance of the definitions of the systemic inflammatory response syndrome and sepsis in neonates. J Perinat Med 2012;40:587–90. - PubMed
-
- Anand R, Leaphart C, Mollen K, Hackam D. The role of the intestinal barrier in the pathogenesis of necrotizing enterocolitis. Shock 2007;27:124–33. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
