

Positive Family History, Infection, Low Absolute Lymphocyte Count (ALC), and Absent Thymic Shadow: Diagnostic Clues for All Molecular Forms of Severe Combined Immunodeficiency (SCID)
- PMID: 25824440
- PMCID: PMC4500664
- DOI: 10.1016/j.jaip.2015.01.026
Positive Family History, Infection, Low Absolute Lymphocyte Count (ALC), and Absent Thymic Shadow: Diagnostic Clues for All Molecular Forms of Severe Combined Immunodeficiency (SCID)
Abstract
Background: Severe combined immunodeficiency (SCID) is a syndrome uniformly fatal during infancy unless recognized and treated successfully by bone marrow transplantation or gene therapy. Because infants with SCID have no abnormal physical appearance, diagnosis is usually delayed unless newborn screening is performed.
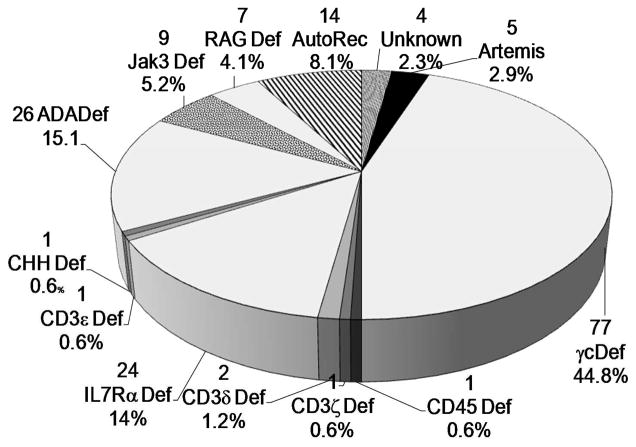
Objective: In this study, we sought to evaluate the presenting features of all 172 patients with SCID transplanted at this institution over the past 31 years.
Methods: We reviewed original charts from 172 consecutive patients with classic SCID who received either T-cell-depleted HLA-haploidentical (N = 154) or HLA-identical (N = 18) nonablative related marrow transplants at Duke University Medical Center from 1982 to 2013.
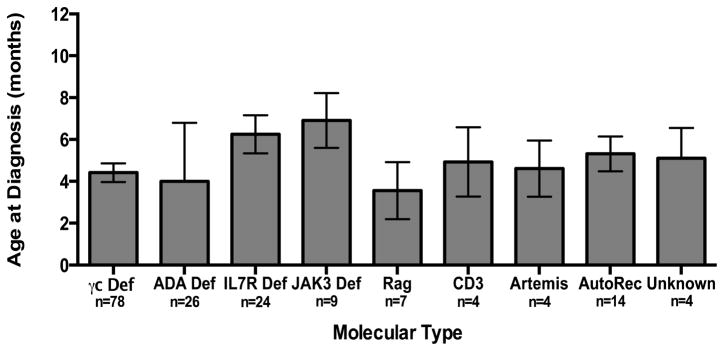
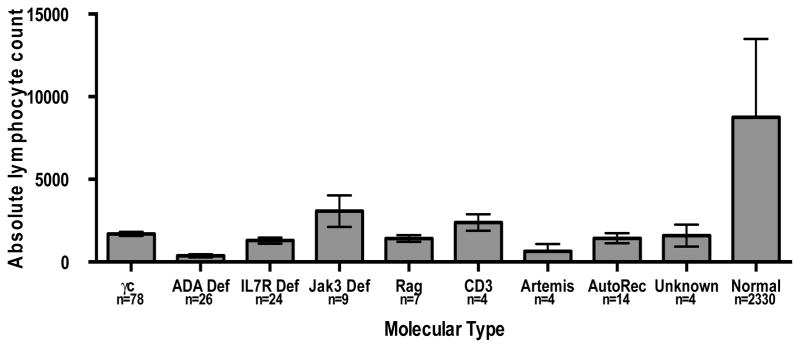
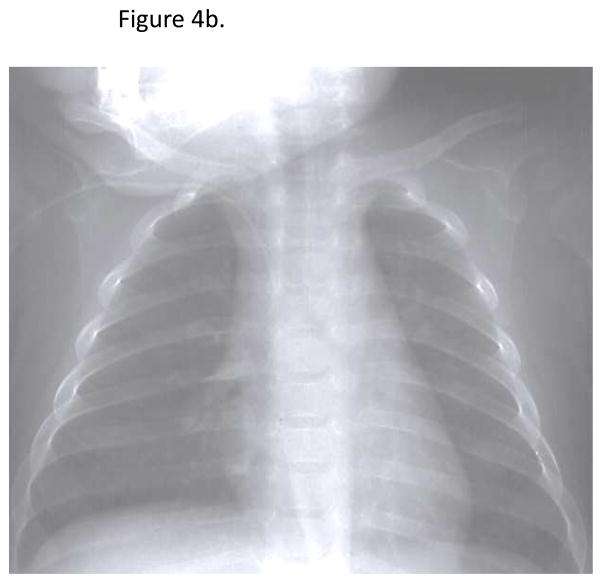
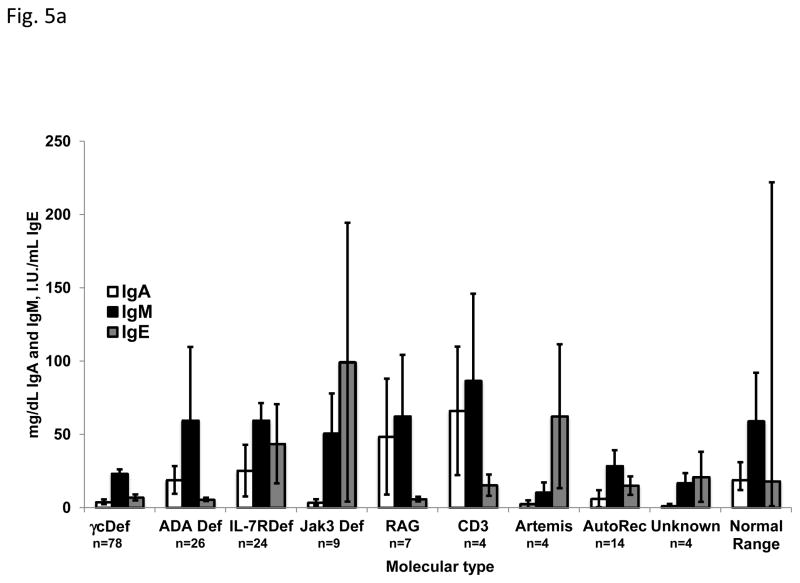
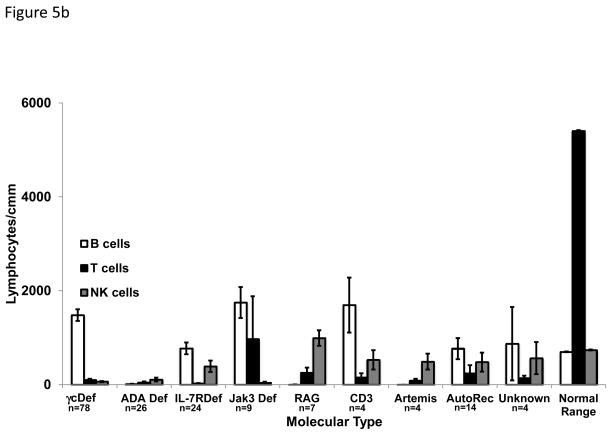
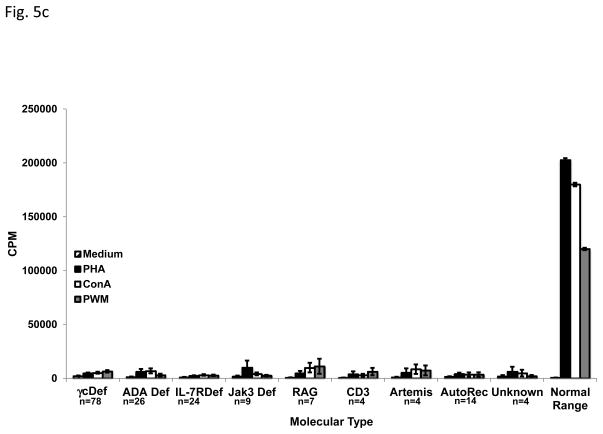
Results: The mean age at presentation was 4.87 months. When there was a family history of early infant death or known SCID (37%), the mean presentation age was much earlier, 2.0 months compared with 6.6 months. Failure to thrive was common, with 84 patients (50%) having a weight less than the 5th percentile. The leading infections included oral moniliasis (43%), viral infections (35.5%), and Pneumocystis jiroveci (26%) pneumonia. The group mean absolute lymphocyte count (ALC) was 1454/cmm; 88% of the infants had an ALC less than 3000/cmm. An absent thymic shadow was seen in 92% of infants with electronic radiographic data available. An absence of T-cell function was found in all patients.
Conclusions: Infants with SCID appear normal at birth but later present with failure to thrive and/or recurrent fungal, viral, and bacterial infections. Low ALCs and an absent thymic shadow on chest x-ray are key diagnostic clues. The absence of T-cell function confirms the diagnosis.
Keywords: Absent thymic shadow; Failure to thrive infections; Lymphopenia; Severe combined immunodeficiency.
Copyright © 2015 American Academy of Allergy, Asthma & Immunology. Published by Elsevier Inc. All rights reserved.
Figures

Comment in
-
While on the Way to Universal Newborn Screening for Severe Combined Immunodeficiency Disease.J Allergy Clin Immunol Pract. 2015 Jul-Aug;3(4):592-3. doi: 10.1016/j.jaip.2015.03.019. J Allergy Clin Immunol Pract. 2015. PMID: 26164577 No abstract available.
References
-
- Buckley RH, Schiff RI, Schiff SE, et al. Human severe combined immunodeficiency: Genetic, phenotypic, and functional diversity in one hundred eight infants. Journal of Pediatrics. 1997;130:378–87. - PubMed
-
- Buckley RH. Molecular defects in human severe combined immunodeficiency and approaches to immune reconstitution. Annual Review of Immunology. 2004;22:625–55. - PubMed
-
- Buckley RH, Schiff SE, Schiff RI, et al. Hematopoietic stem-cell transplantation for the treatment of severe combined immunodeficiency. New Engl J Med. 1999;340:508–16. - PubMed
-
- Noguchi M, Yi HF, Rosenblatt HM, et al. Interleukin-2 Receptor Gamma Chain Mutation Results in X-Linked Severe Combined Immunodeficiency in Humans. Cell. 1993;73:147–57. - PubMed
-
- Russell SM, Keegan AD, Harada N, et al. Interleukin-2 Receptor Gamma- Chain - a Functional Component of the Interleukin-4 Receptor. Science. 1993;262:1880–83. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
