

Comparison of Subdural Hematoma Risk between Hemodialysis and Peritoneal Dialysis Patients with ESRD
- PMID: 25825482
- PMCID: PMC4455210
- DOI: 10.2215/CJN.08140814
Comparison of Subdural Hematoma Risk between Hemodialysis and Peritoneal Dialysis Patients with ESRD
Abstract
Background and objectives: This study compared the risk of subdural hematoma (SDH) and subsequent mortality in hemodialysis (HD) and peritoneal dialysis (PD) patients with ESRD.
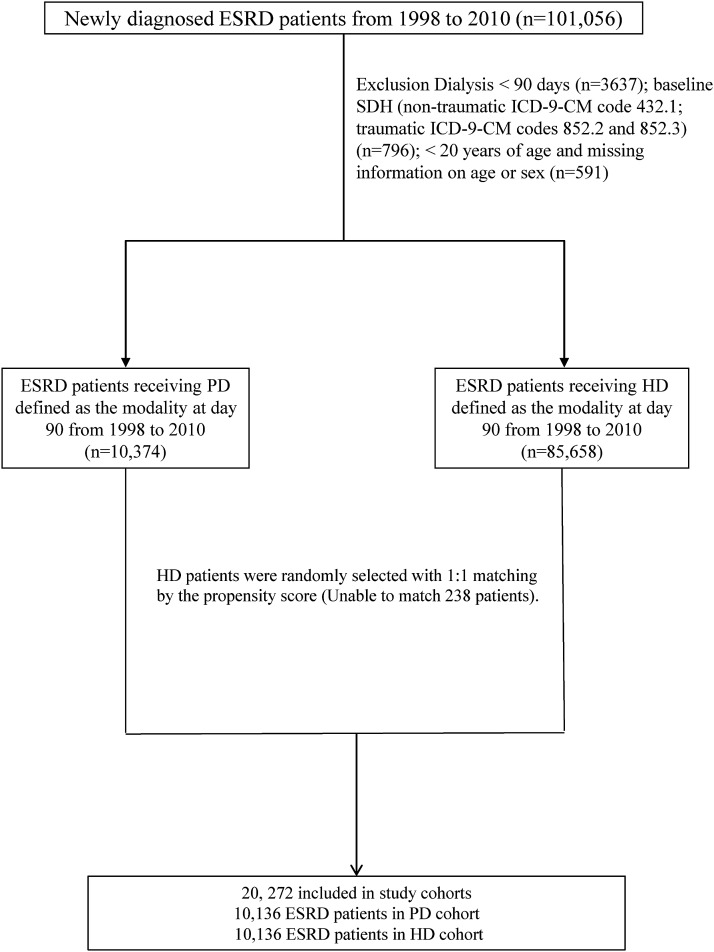
Design, setting, participants, & measurements: Claims data were obtained from the National Health Insurance Administration Research Database in Taiwan. This retrospective cohort study comprised 10,136 PD patients and 10,136 HD patients with newly diagnosed ESRD from 1998 to 2010. Patients were matched by propensity score and year of dialysis initiation. Incidence rates and hazard ratios of SDH as well as odds ratios of subsequent 30-day deaths from SDH were evaluated from the date of the first dialysis session to the date when SDH was diagnosed, or the date of renal transplantation, death, withdraw from insurance, or the end of the follow-up period (December 31, 2011).
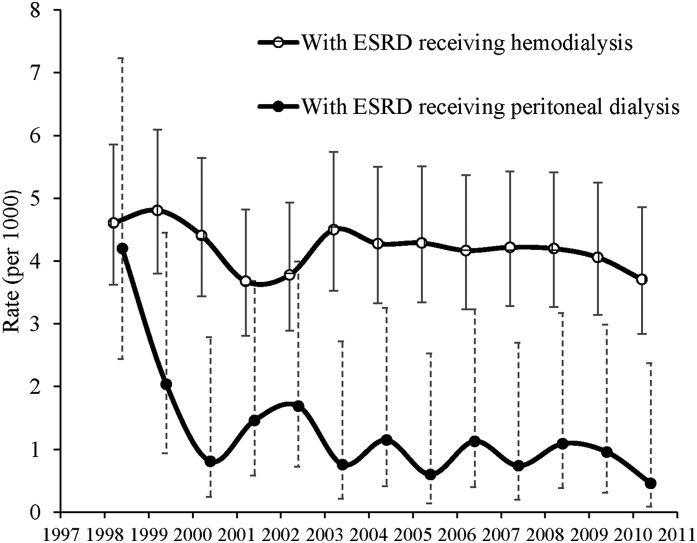
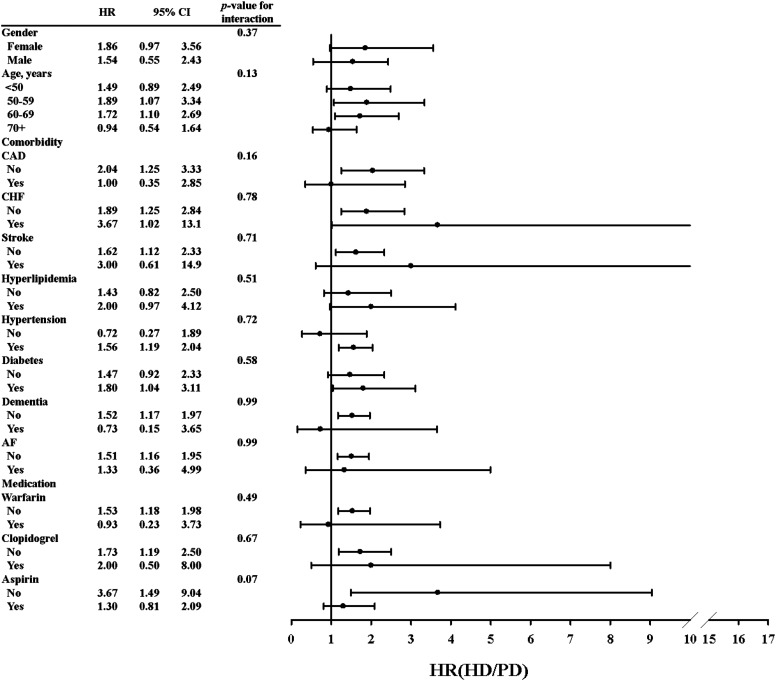
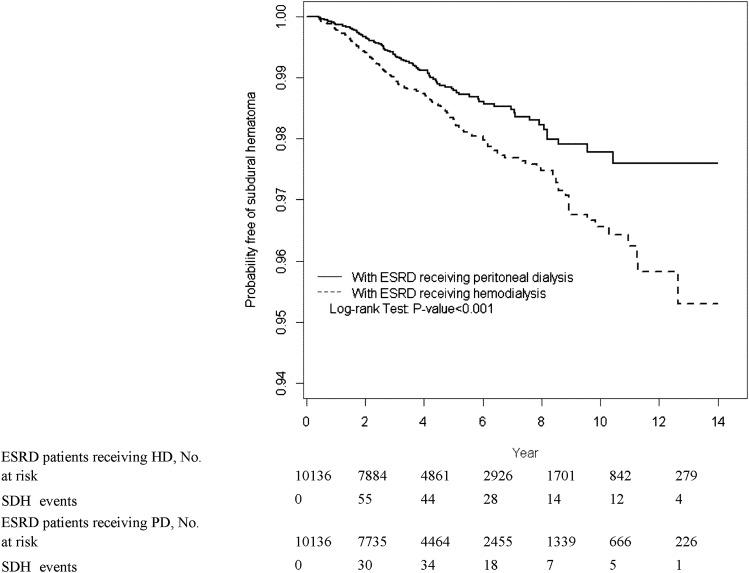
Results: Median (25th percentile, 75th percentile) follow-up times for SDH events were 3.61 years (1.91, 6.33) and 3.33 years (1.83, 5.66) in the HD and PD cohorts, respectively. The overall SDH incidence rate (95% confidence interval [95% CI]) was 61.4% higher in the HD cohort than in the PD cohort (34.7 [95% CI, 31.4 to 35.4] versus 21.5 [95% CI, 20.2 to 22.9] per 10,000 person-years, with an adjusted hazard ratio of 1.62 [95% CI, 1.17 to 2.33]). Approximately 152 of 253 (60%) of SDH events were associated with trauma. Subsequent 30-day SDH-related mortality was not statistically higher in HD patients than in PD patients (29.1% versus 25.3%; adjusted odds ratio, 1.30; 95% CI, 0.70 to 2.41).
Conclusions: HD patients have a higher risk of developing SDH than PD patients. Both patient groups have a high risk of mortality. Routine education on fall prevention is needed for dialysis patients.
Keywords: ESRD; hemodialysis; mortality; peritoneal dialysis; subdural hematoma.
Copyright © 2015 by the American Society of Nephrology.
Figures
References
-
- Harvey LA, Close JC: Traumatic brain injury in older adults: Characteristics, causes and consequences. Injury 43: 1821–1826, 2012 - PubMed
-
- Jacobsson LJ, Westerberg M, Lexell J: Demographics, injury characteristics and outcome of traumatic brain injuries in northern Sweden. Acta Neurol Scand 116: 300–306, 2007 - PubMed
-
- Maxeiner H, Wolff M: Pure subdural hematomas: A postmortem analysis of their form and bleeding points. Neurosurgery 50: 503–508, discussion 508–509, 2002 - PubMed
-
- Gottesman RF, Komotar R, Hillis AE: Neurologic aspects of traumatic brain injury. Int Rev Psychiatry 15: 302–309, 2003 - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Medical
