

Motivational interviewing and dietary counseling for obesity in primary care: an RCT
- PMID: 25825539
- PMCID: PMC4379459
- DOI: 10.1542/peds.2014-1880
Motivational interviewing and dietary counseling for obesity in primary care: an RCT
Abstract
Background and objective: Few studies have tested the impact of motivational interviewing (MI) delivered by primary care providers on pediatric obesity. This study tested the efficacy of MI delivered by providers and registered dietitians (RDs) to parents of overweight children aged 2 through 8.
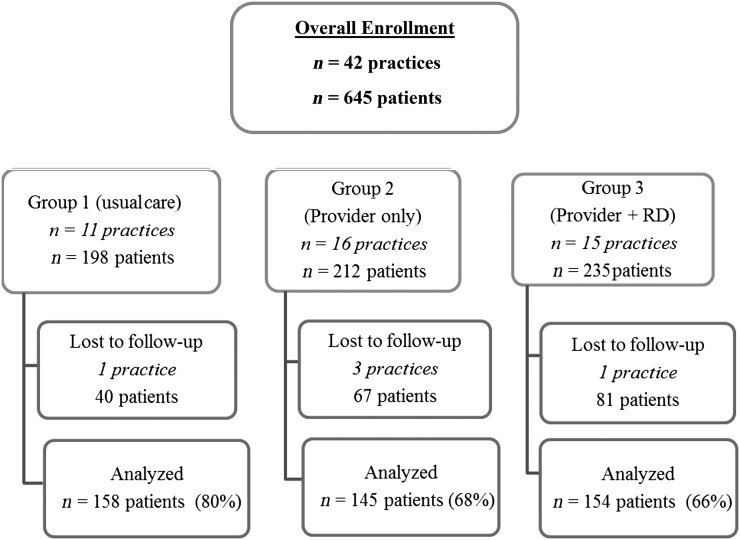
Methods: Forty-two practices from the Pediatric Research in Office Settings Network of the American Academy of Pediatrics were randomly assigned to 1 of 3 groups. Group 1 (usual care) measured BMI percentile at baseline and 1- and 2-year follow-up. Group 2 (provider only) delivered 4 MI counseling sessions to parents of the index child over 2 years. Group 3 (provider + RD) delivered 4 provider MI sessions plus 6 MI sessions from a RD. The primary outcome was child BMI percentile at 2-year follow up.
Results: At 2-year follow-up, the adjusted BMI percentile was 90.3, 88.1, and 87.1 for groups 1, 2, and 3, respectively. The group 3 mean was significantly (P = .02) lower than group 1. Mean changes from baseline in BMI percentile were 1.8, 3.8, and 4.9 across groups 1, 2, and 3.
Conclusions: MI delivered by providers and RDs (group 3) resulted in statistically significant reductions in BMI percentile. Research is needed to determine the clinical significance and persistence of the BMI effects observed. How the intervention can be brought to scale (in particular, how to train physicians to use MI effectively and how best to train RDs and integrate them into primary care settings) also merits future research.
Trial registration: ClinicalTrials.gov NCT01335308.
Keywords: obesity.
Copyright © 2015 by the American Academy of Pediatrics.
Comment in
-
Primary care interventions for pediatric obesity: need for an integrated approach.Pediatrics. 2015 Apr;135(4):757-8. doi: 10.1542/peds.2015-0495. Pediatrics. 2015. PMID: 25825541 No abstract available.
References
-
- Lee WW. An overview of pediatric obesity. Pediatr Diabetes. 2007;8(suppl 9):76–87 - PubMed
-
- Institute of Medicine. Accelerating Progress in Obesity Prevention: Solving the Weight of the Nation. Washington, DC: The National Academies Press; 2012 - PubMed
-
- Story MT, Neumark-Stzainer DR, Sherwood NE, et al. Management of child and adolescent obesity: attitudes, barriers, skills, and training needs among health care professionals. Pediatrics. 2002;110(1):210–214 - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
