

Endoscopic enucleation versus open prostatectomy for treating large benign prostatic hyperplasia: a meta-analysis of randomized controlled trials
- PMID: 25826453
- PMCID: PMC4380430
- DOI: 10.1371/journal.pone.0121265
Endoscopic enucleation versus open prostatectomy for treating large benign prostatic hyperplasia: a meta-analysis of randomized controlled trials
Abstract
Objectives: To evaluate the overall efficacy and safety of endoscopic enucleation of the prostate (EP) vs open prostatectomy (OP) for large benign prostatic hyperplasia (BPH).
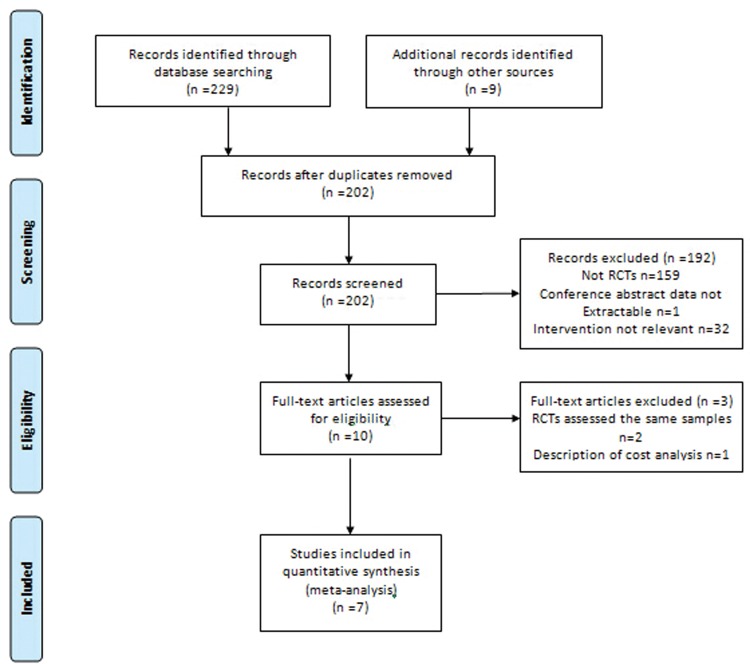
Methods: We conducted an electronic search of PubMed/Medline, EMBASE, The Cochrane Library, and Web of Science to detect all relevant randomized controlled trials (RCTs) comparing EP with OP. A meta-analysis was performed using Review Manager 5.3.
Results: Seven RCTs (735 patients) were included. At the 3-, 6- and 12-month follow-up, there were no significant differences in the International Prostate Symptom Score (IPSS), maximum flow rate (Qmax), quality of life (QoL) score and post-void residual urine volume (PVR) between EP and OP. The International Index of Erectile Function (IIEF-5) was higher with EP (weighted mean difference [WMD]: 1.00, 95% confidence interval [CI]: 0.21 to 1.78, p=0.01) at the 12-month follow-up. The catheterization time (WMD: 3.80 d, 95%CI: -5.11 to -2.48, P<0.00001) and hospital stay (WMD: 4.93 d, 95%CI: -5.96 to -3.89, P<0.00001) were shorter with EP. The duration of operation was longer for EP compared with OP (WMD: 16.21 min, 95%CI: 3.72 to 28.70, P=0.01). The resected tissue weight (WMD: -9.63 g, 95%CI: -14.46 to -4.81, P<0.0001) and decrease in hemoglobin (WMD: -1.14 g/dL, 95%CI: -1.81 to -0.47, P=0.0008) were less with EP. EP was associated with fewer blood transfusions (risk ratio: 0.22, 95%CI: 0.10 to 0.47, P=0.0001). There were no significant differences between EP and OP when comparing other complications.
Conclusions: Although only a limited number of RCTs with relatively limited follow-up are available, EP is shown to have a similar postoperative profile and comparable safety to OP. By contrast, EP may have a more desirable perioperative profile. EP appears to be an effective and safe minimally invasive option for treating large prostates that requires only brief convalescence.
Conflict of interest statement
Figures
References
-
- McConnell JD. The pathophysiology of benign prostatic hyperplasia. J Androl. 1991; 12: 356–363. - PubMed
-
- Girman CJ, Jacobsen SJ, Tsukamoto T, Richard F, Garraway WM, Sagnier PP, et al. Health-related quality of life associated with lower urinary tract symptoms in four countries. Urology. 1998; 51: 428–436. - PubMed
-
- Welch G, Weinger K, Barry MJ. Quality-of-life impact of lower urinary tract symptom severity: results from the Health Professionals Follow-up Study. Urology. 2002; 59: 245–250. - PubMed
-
- Gu FL, Xia TL, Kong XT. Preliminary study of the frequency of benign prostatic hyperplasia and prostatic cancer in China. Urology. 1994; 44: 688–691. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
