

Spectral analysis-based risk score enables early prediction of mortality and cerebral performance in patients undergoing therapeutic hypothermia for ventricular fibrillation and comatose status
- PMID: 25828128
- PMCID: PMC5568426
- DOI: 10.1016/j.ijcard.2015.03.074
Spectral analysis-based risk score enables early prediction of mortality and cerebral performance in patients undergoing therapeutic hypothermia for ventricular fibrillation and comatose status
Abstract
Background: Early prognosis in comatose survivors after cardiac arrest due to ventricular fibrillation (VF) is unreliable, especially in patients undergoing mild hypothermia. We aimed at developing a reliable risk-score to enable early prediction of cerebral performance and survival.
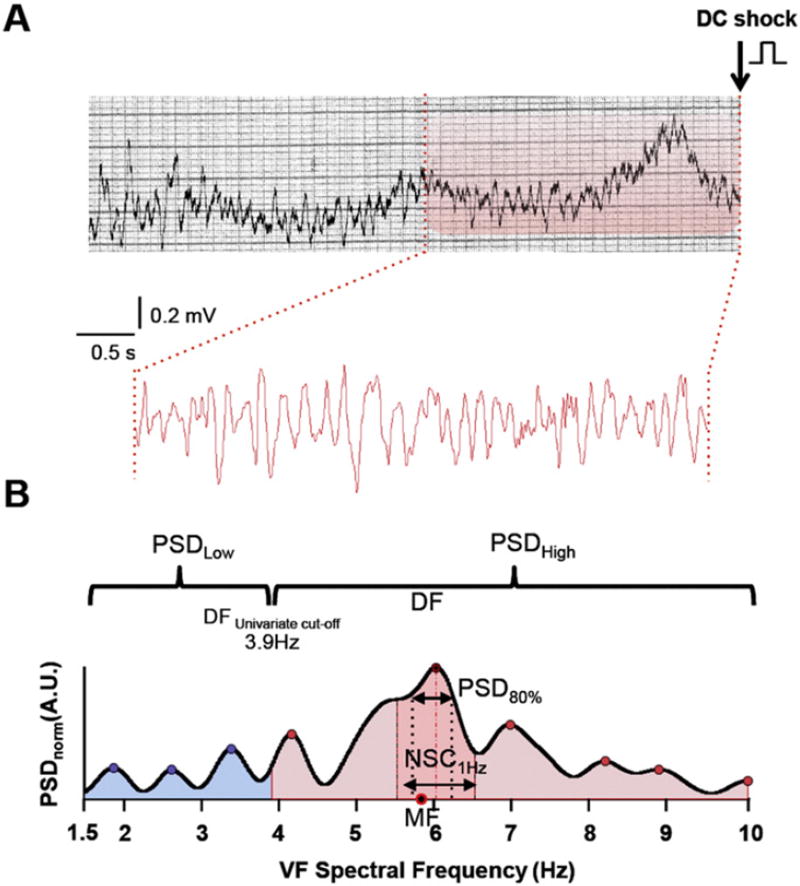
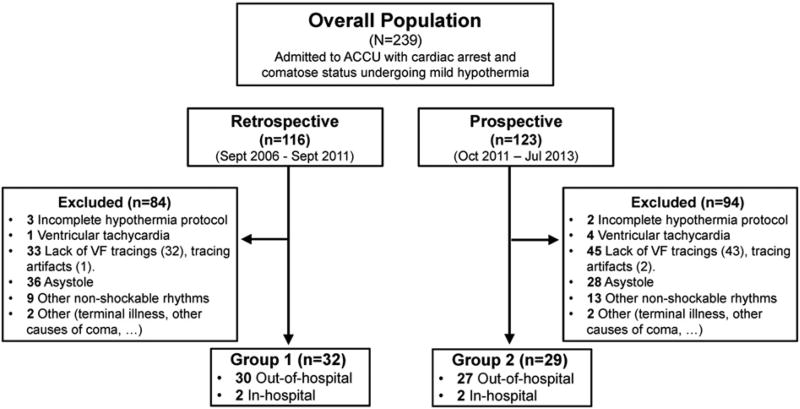
Methods: Sixty-one out of 239 consecutive patients undergoing mild hypothermia after cardiac arrest, with eventual return of spontaneous circulation (ROSC), and comatose status on admission fulfilled the inclusion criteria. Background clinical variables, VF time and frequency domain fundamental variables were considered. The primary and secondary outcomes were a favorable neurological performance (FNP) during hospitalization and survival to hospital discharge, respectively. The predictive model was developed in a retrospective cohort (n = 32; September 2006-September 2011, 48.5 ± 10.5 months of follow-up) and further validated in a prospective cohort (n = 29; October 2011-July 2013, 5 ± 1.8 months of follow-up).
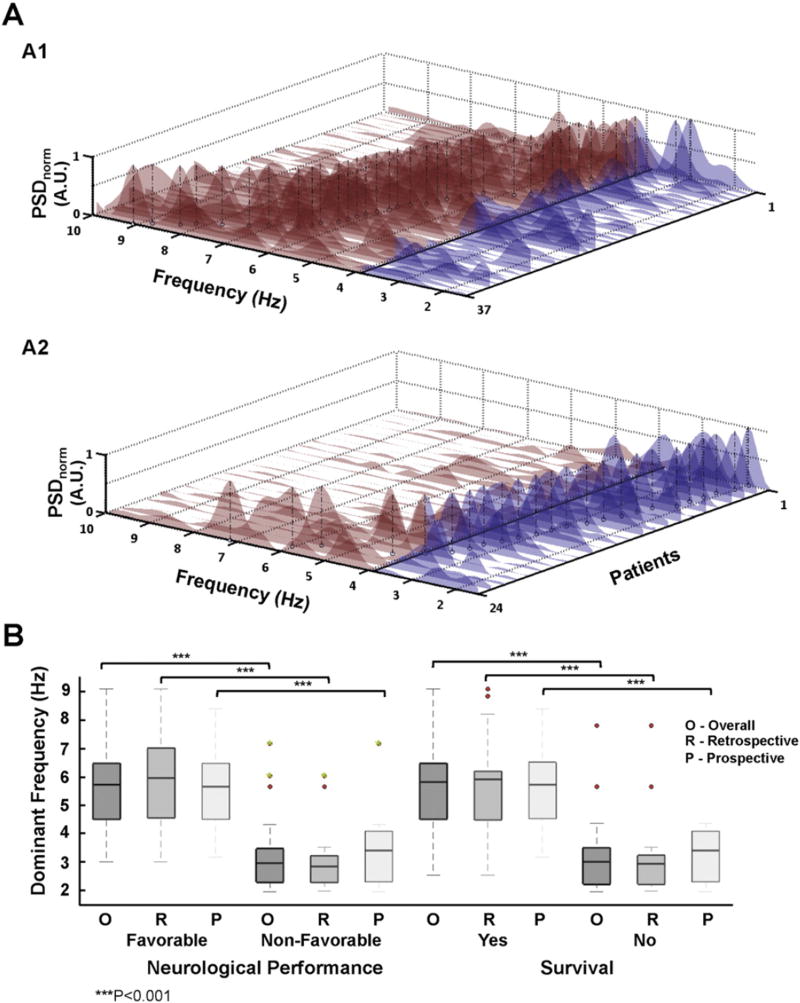
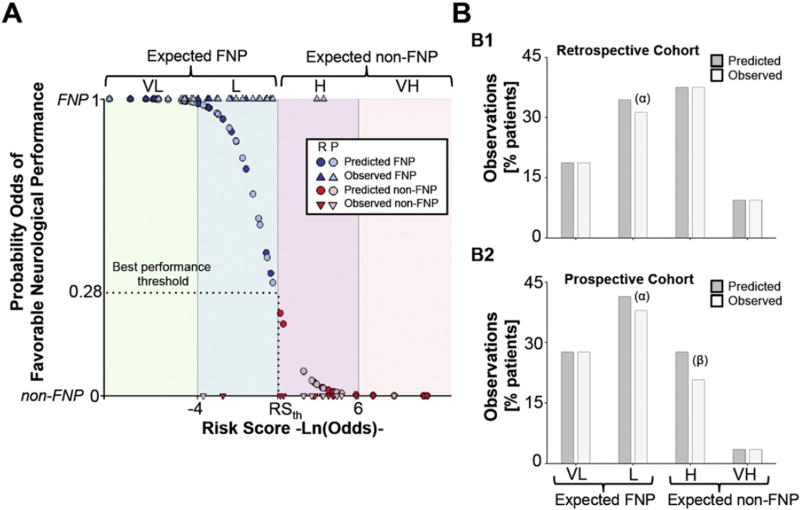
Results: FNP was present in 16 (50.0%) and 21 patients (72.4%) in the retrospective and prospective cohorts, respectively. Seventeen (53.1%) and 21 patients (72.4%), respectively, survived to hospital discharge. Both outcomes were significantly associated (p < 0.001). Retrospective multivariate analysis provided a prediction model (sensitivity = 0.94, specificity = 1) that included spectral dominant frequency, derived power density and peak ratios between high and low frequency bands, and the number of shocks delivered before ROSC. Validation on the prospective cohort showed sensitivity = 0.88 and specificity = 0.91. A model-derived risk-score properly predicted 93% of FNP. Testing the model on follow-up showed a c-statistic ≥ 0.89.
Conclusions: A spectral analysis-based model reliably correlates time-dependent VF spectral changes with acute cerebral injury in comatose survivors undergoing mild hypothermia after cardiac arrest.
Keywords: Cardiac arrest; Cerebral injury; Dominant frequency; Early prognosis; Ventricular fibrillation.
Copyright © 2015 Elsevier Ireland Ltd. All rights reserved.
Conflict of interest statement
None.
Figures
References
-
- Nadkarni VM, Larkin GL, Peberdy MA, Carey SM, Kaye W, Mancini ME, et al. First documented rhythm and clinical outcome from in-hospital cardiac arrest among children and adults. JAMA. 2006;295:50–57. - PubMed
-
- Cobb LA, Fahrenbruch CE, Olsufka M, Copass MK. Changing incidence of out-of-hospital ventricular fibrillation, 1980–2000. JAMA. 2002;288:3008–3013. - PubMed
-
- Sugawara T, Chan PH. Reactive oxygen radicals and pathogenesis of neuronal death after cerebral ischemia. Antioxid. Redox Signal. 2003;5:597–607. - PubMed
-
- Bernard SA, Gray TW, Buist MD, Jones BM, Silvester W, Gutteridge G, et al. Treatment of comatose survivors of out-of-hospital cardiac arrest with induced hypothermia. N. Engl. J. Med. 2002;346:557–563. - PubMed
-
- Mild therapeutic hypothermia to improve the neurologic outcome after cardiac arrest. N. Engl. J. Med. 2002;346:549–556. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
