

Common normal variants of pediatric vertebral development that mimic fractures: a pictorial review from a national longitudinal bone health study
- PMID: 25828359
- PMCID: PMC4519278
- DOI: 10.1007/s00247-014-3210-y
Common normal variants of pediatric vertebral development that mimic fractures: a pictorial review from a national longitudinal bone health study
Abstract
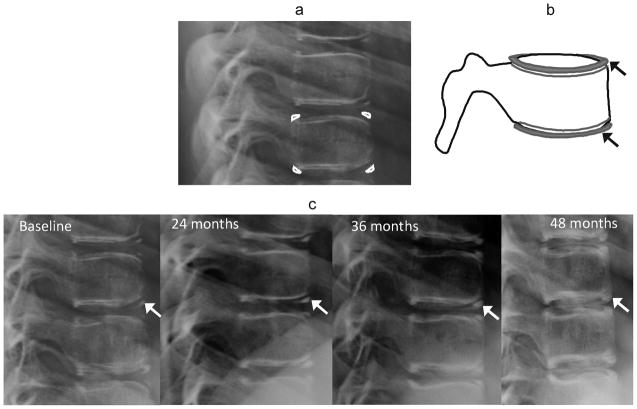
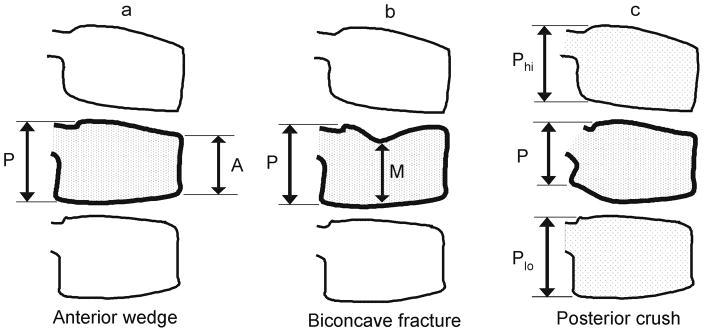
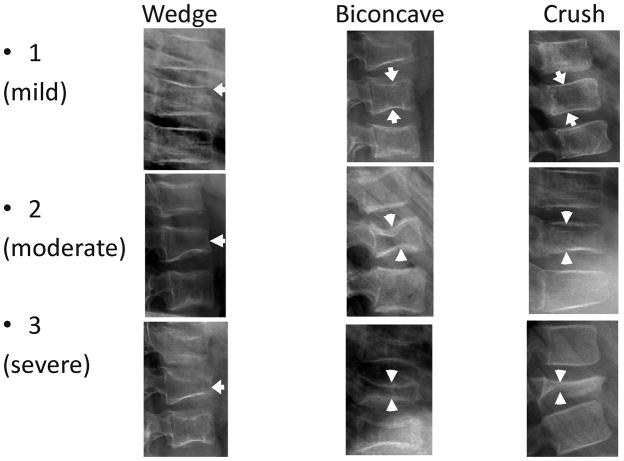
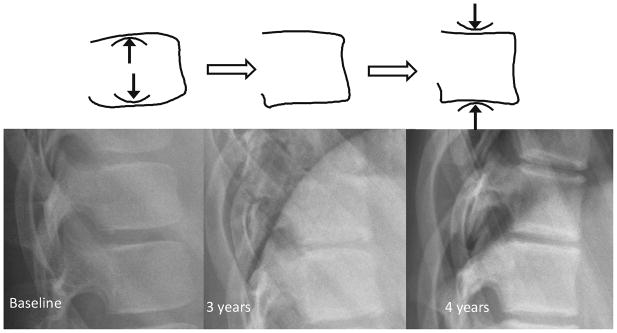
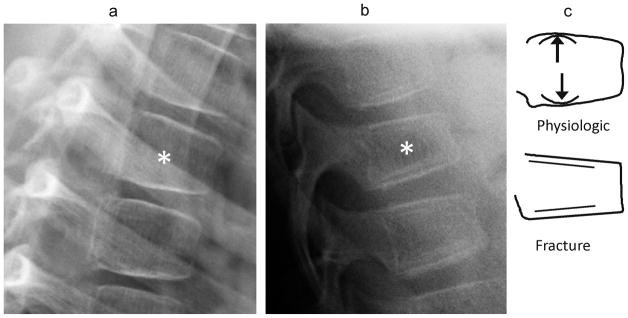
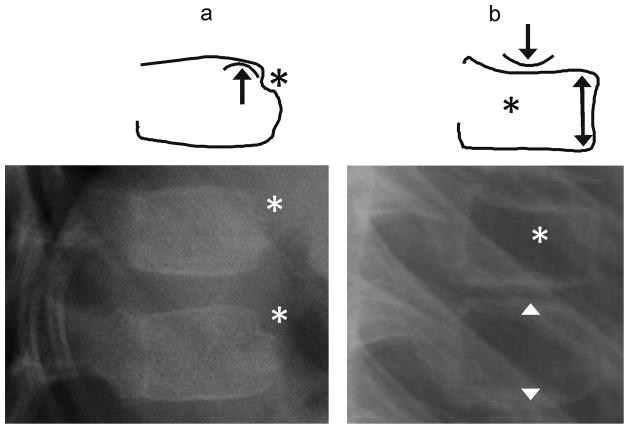
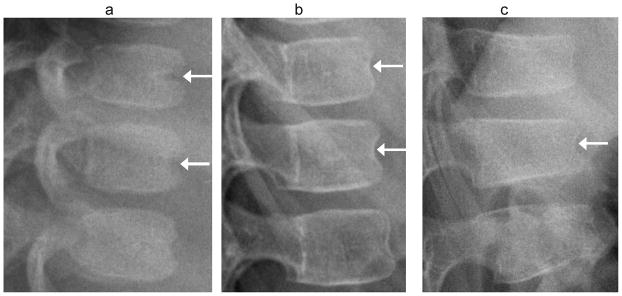
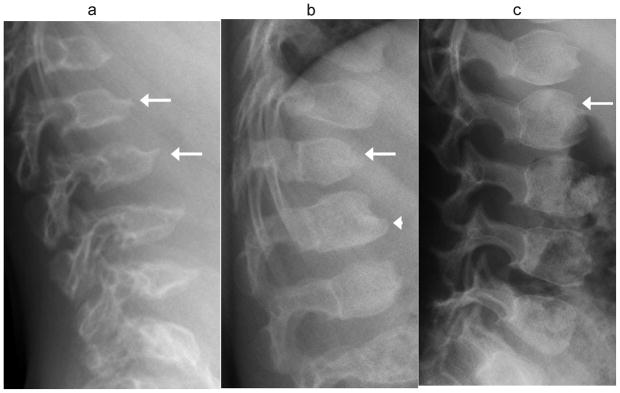
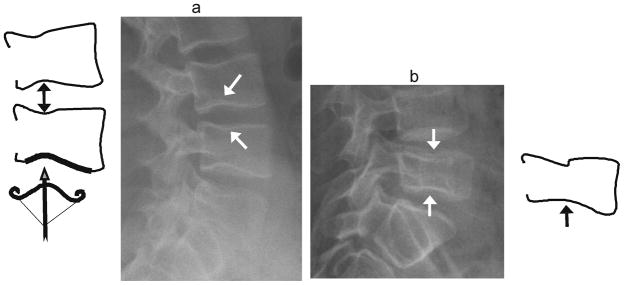
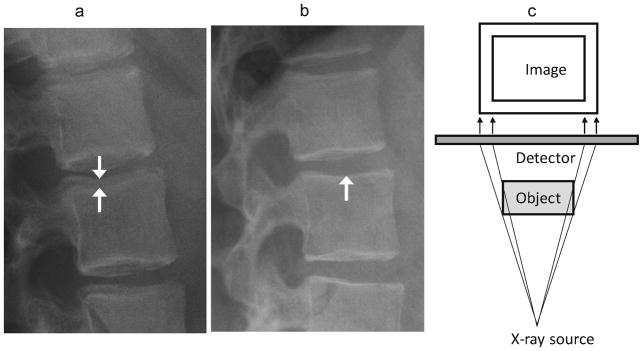
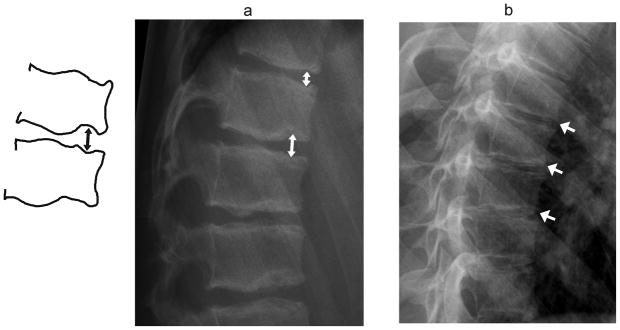
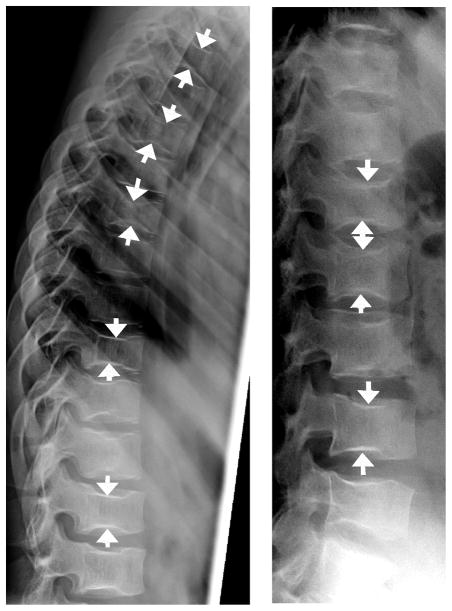
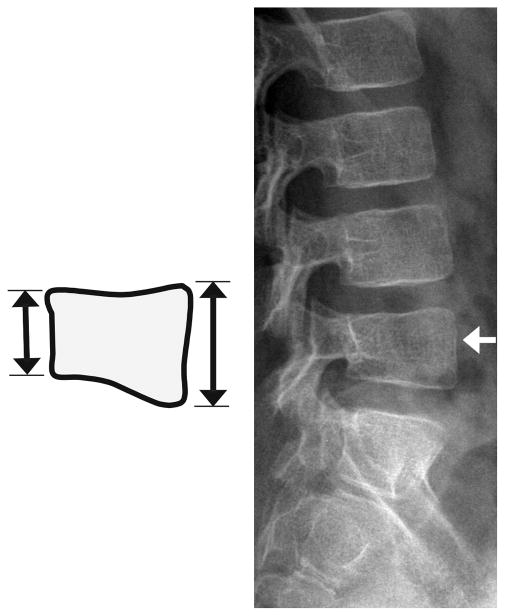
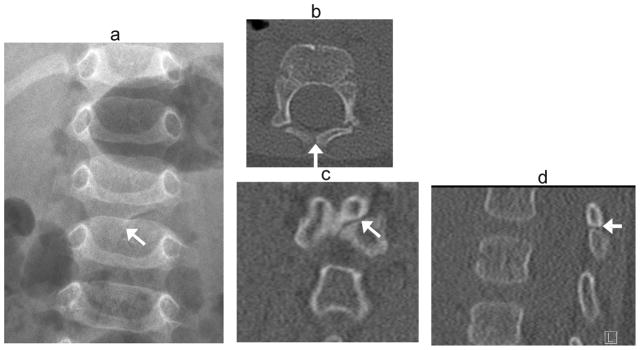
Children with glucocorticoid-treated illnesses are at risk for osteoporotic vertebral fractures, and growing awareness of this has led to increased monitoring for these fractures. However scant literature describes developmental changes in vertebral morphology that can mimic fractures. The goal of this paper is to aid in distinguishing between normal variants and fractures. We illustrate differences using lateral spine radiographs obtained annually from children recruited to the Canada-wide STeroid-Associated Osteoporosis in the Pediatric Population (STOPP) observational study, in which 400 children with glucocorticoid-treated leukemia, rheumatic disorders, and nephrotic syndrome were enrolled near glucocorticoid initiation and followed prospectively for 6 years. Normal variants mimicking fractures exist in all regions of the spine and fall into two groups. The first group comprises variants mimicking pathological vertebral height loss, including not-yet-ossified vertebral apophyses superiorly and inferiorly, which can lead to a vertebral shape easily over-interpreted as anterior wedge fracture, physiological beaking, or spondylolisthesis associated with shortened posterior vertebral height. The second group includes variants mimicking other radiologic signs of fractures: anterior vertebral artery groove resembling an anterior buckle fracture, Cupid's bow balloon disk morphology, Schmorl nodes mimicking concave endplate fractures, and parallax artifact resembling endplate interruption or biconcavity. If an unexpected vertebral body contour is detected, careful attention to its location, detailed morphology, and (if available) serial changes over time may clarify whether it is a fracture requiring change in management or simply a normal variant. Awareness of the variants described in this paper can improve accuracy in the diagnosis of pediatric vertebral fractures.
Conflict of interest statement
Figures
References
-
- Leroux J, Vivier PH, Ould Slimane M, Foulongne E, Abu-Amara S, Lechevallier J, Griffet J. Early diagnosis of thoracolumbar spine fractures in children. A prospective study. Orthop Traumatol Surg Res. 2013;99:60–65. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
