

Meta-analysis of predictive clinicopathologic factors for lymph node metastasis in patients with early colorectal carcinoma
- PMID: 25829807
- PMCID: PMC4366960
- DOI: 10.3346/jkms.2015.30.4.398
Meta-analysis of predictive clinicopathologic factors for lymph node metastasis in patients with early colorectal carcinoma
Abstract
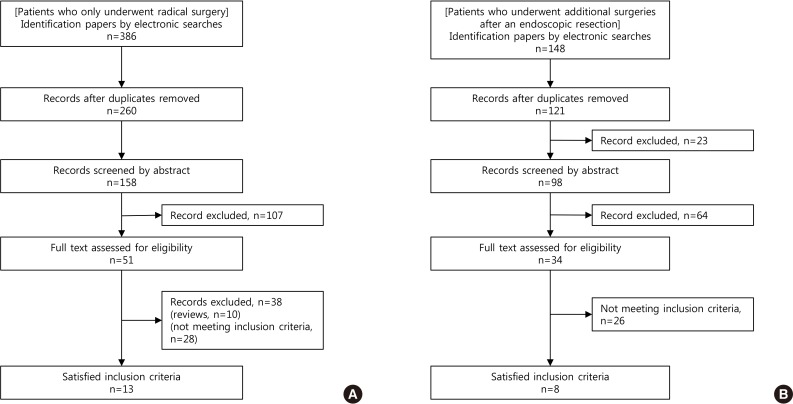
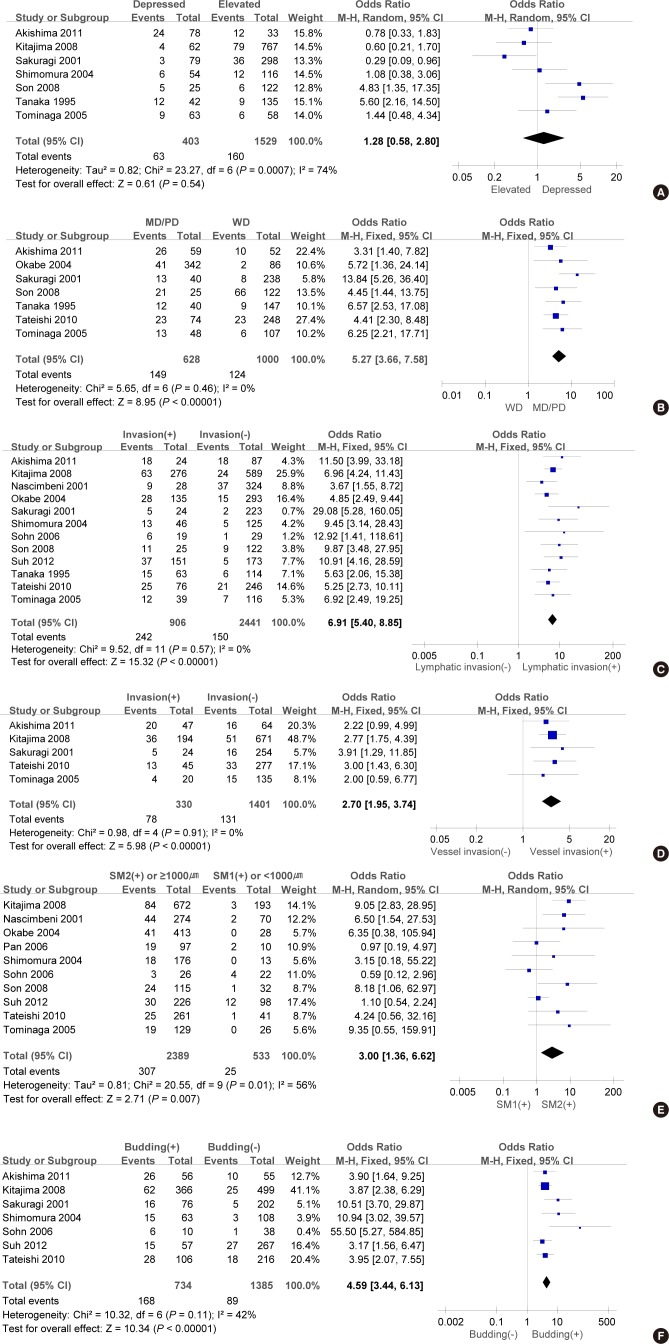
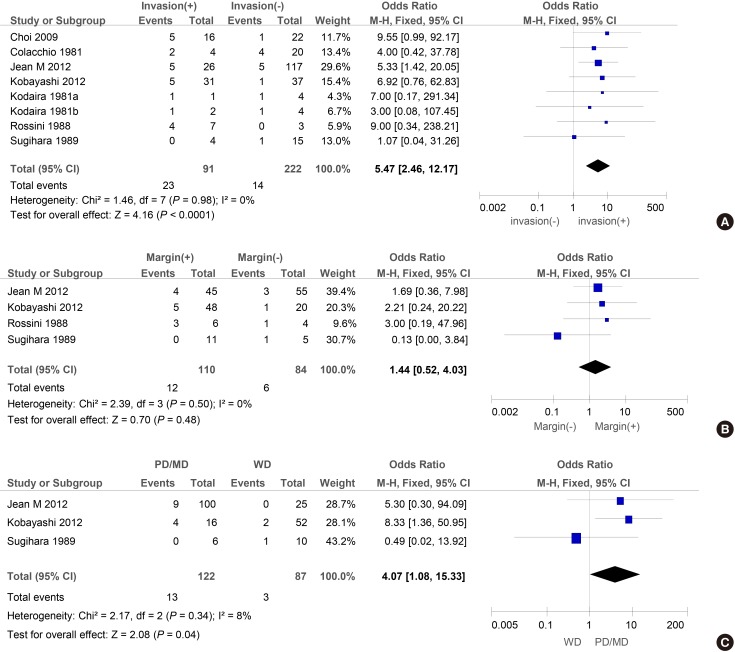
The objective of this study was to conduct a meta-analysis to determine risk factors that may facilitate patient selection for radical resections or additional resections after a polypectomy. Eligible articles were identified by searches of PUBMED, Cochrane Library and Korean Medical Database using the terms (early colorectal carcinoma [ECC], lymph node metastasis [LNM], colectomy, endoscopic resection). Thirteen cohort studies of 7,066 ECC patients who only underwent radical surgery have been analysed. There was a significant risk of LNM when they had submucosal invasion (≥ SM2 or ≥ 1,000 µm) (odds Ratio [OR], 3.00; 95% confidence interval [CI], 1.36-6.62, P = 0.007). Moreover, it has been found that vascular invasion (OR, 2.70; 95% CI, 1.95-3.74; P < 0.001), lymphatic invasion (OR, 6.91; 95% CI, 5.40-8.85; P < 0.001), poorly differentiated carcinomas (OR, 8.27; 95% CI, 4.67-14.66; P < 0.001) and tumor budding (OR, 4.59; 95% CI, 3.44-6.13; P < 0.001) were significantly associated with LNM. Furthermore, another analysis was carried out on eight cohort studies of 310 patients who underwent additional surgeries after an endoscopic resection. The major factors identified in these studies include lymphovascular invasion on polypectomy specimens (OR, 5.47; 95% CI, 2.46-12.17; P < 0.001) and poorly or moderately differentiated carcinomas (OR, 4.07; 95% CI, 1.08-15.33; P = 0.04). For ECC patients with ≥ SM2 or ≥ 1,000 µm submucosal invasion, vascular invasion, lymphatic invasion, poorly differentiated carcinomas or tumor budding, it is deemed that a more extensive resection accompanied by a lymph node dissection is necessary. Even if the lesion is completely removed by an endoscopic resection, an additional surgical resection should be considered in patients with poorly or moderately differentiated carcinomas or lymphovascular invasion.
Keywords: Colectomy; Colorectal Neoplasms; Endoscopy; Lymph Nodes.
Conflict of interest statement
The authors have no potential conflicts of interest to disclose.
Figures
References
-
- Sobin LH, Wittekind C International Union against Cancer. TNM : classification of malignant tumours. 6th ed. New York: Wiley-Liss; 2002.
-
- Kyzer S, Bégin LR, Gordon PH, Mitmaker B. The care of patients with colorectal polyps that contain invasive adenocarcinoma. Endoscopic polypectomy or colectomy? Cancer. 1992;70:2044–2050. - PubMed
-
- Minamoto T, Mai M, Ogino T, Sawaguchi K, Ohta T, Fujimoto T, Takahashi Y. Early invasive colorectal carcinomas metastatic to the lymph node with attention to their nonpolypoid development. Am J Gastroenterol. 1993;88:1035–1039. - PubMed
-
- Tanaka S, Haruma K, Teixeira CR, Tatsuta S, Ohtsu N, Hiraga Y, Yoshihara M, Sumii K, Kajiyama G, Shimamoto F. Endoscopic treatment of submucosal invasive colorectal carcinoma with special reference to risk factors for lymph node metastasis. J Gastroenterol. 1995;30:710–717. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
