

Multi-capillary column-ion mobility spectrometry (MCC-IMS) as a new method for the quantification of occupational exposure to sevoflurane in anaesthesia workplaces: an observational feasibility study
- PMID: 25829942
- PMCID: PMC4379543
- DOI: 10.1186/s12995-015-0056-7
Multi-capillary column-ion mobility spectrometry (MCC-IMS) as a new method for the quantification of occupational exposure to sevoflurane in anaesthesia workplaces: an observational feasibility study
Abstract
Background: Occupational exposure to sevoflurane has the potential to cause health damage in hospital personnel. Workplace contamination with the substance mostly is assessed by using photoacoustic infrared spectrometry with detection limits of 10 ppbv. Multi-capillary column-ion mobility spectrometry (MCC-IMS) could be an alternative technology for the quantification of sevoflurane in the room air and could be even more accurate because of potentially lower detection limits. The aim of this study was to test the hypothesis that MCC-IMS is able to detect and monitor very low concentrations of sevoflurane (<10 ppbv) and to evaluate the exposure of hospital personnel to sevoflurane during paediatric anaesthesia and in the post anaesthesia care unit (PACU).
Methods: A MCC-IMS device was calibrated to several concentrations of sevoflurane and limits of detection (LOD) and quantification (LOQ) were calculated. Sevoflurane exposure of hospital personnel was measured at two anaesthesia workplaces and time-weighted average (TWA) values were calculated.
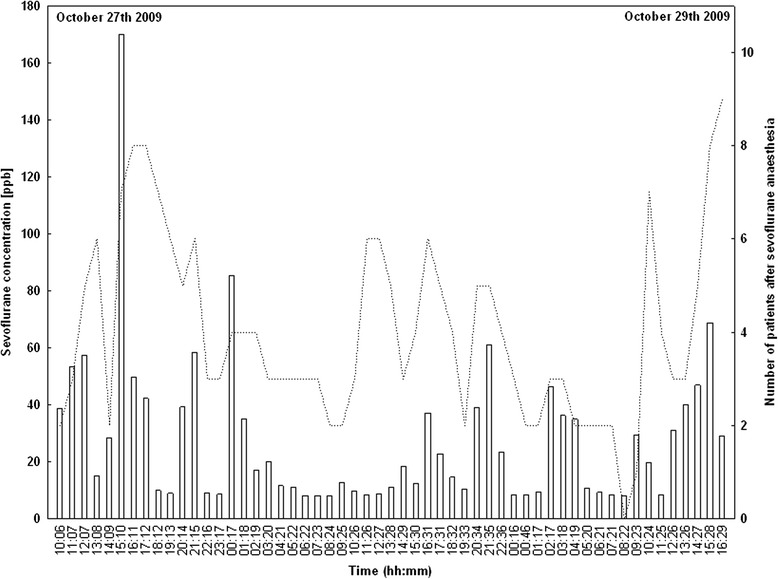
Results: The LOD was 0.0068 ppbv and the LOQ was 0.0189 ppbv. During paediatric anaesthesia the mean sevoflurane concentration was 46.9 ppbv (8.0 - 314.7 ppbv) with TWA values between 5.8 and 45.7 ppbv. In the PACU the mean sevoflurane concentration was 27.9 ppbv (8.0 - 170.2 ppbv) and TWA values reached from 8.3 to 45.1 ppbv.
Conclusions: MCC-IMS shows a significantly lower LOD and LOQ than comparable methods. It is a reliable technology for monitoring sevoflurane concentrations at anaesthesia workplaces and has a particular strength in quantifying low-level contaminations of sevoflurane. The exposure of the personnel working in these areas did not exceed recommended limits and therefore adverse health effects are unlikely.
Keywords: Ion mobility spectrometry; Limit of detection; Occupational exposure; Room air analyses; Sevoflurane; Volatile anaesthetics.
Figures



References
LinkOut - more resources
Full Text Sources
Other Literature Sources
