

Review
doi: 10.3978/j.issn.2078-6891.2014.065.
Non-operative therapies for colorectal liver metastases
Affiliations
- PMID: 25830041
- PMCID: PMC4311101
- DOI: 10.3978/j.issn.2078-6891.2014.065
Item in Clipboard
Review
Non-operative therapies for colorectal liver metastases
J Gastrointest Oncol.
2015 Apr.
Abstract
Locoregional therapies for colorectal liver metastases complement systemic therapy by providing an opportunity for local control of hepatic spread. The armamentarium for liver-directed therapy includes ablative therapies, embolization, and stereotactic body radiation therapy. At this time, prospective studies comparing these modalities are limited and decision-making relies on a multidisciplinary approach for optimal patient management. Herein, we describe multiple therapeutic non-surgical procedures and an overview of the results of these treatments.
Keywords: Colon cancer; ablation; embolization; liver metastases; radiation.
Figures
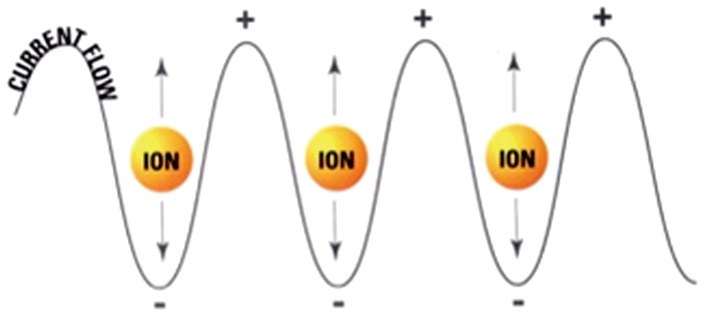
Mechanism of radiofrequency ablation (RFA). Rapidly alternating electrical current produces ionic oscillations in bipolar water molecules, which generate frictional heat.

RFA electrode probe. RFA, radiofrequency ablation.
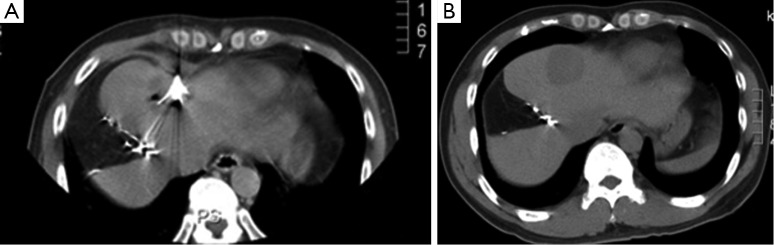
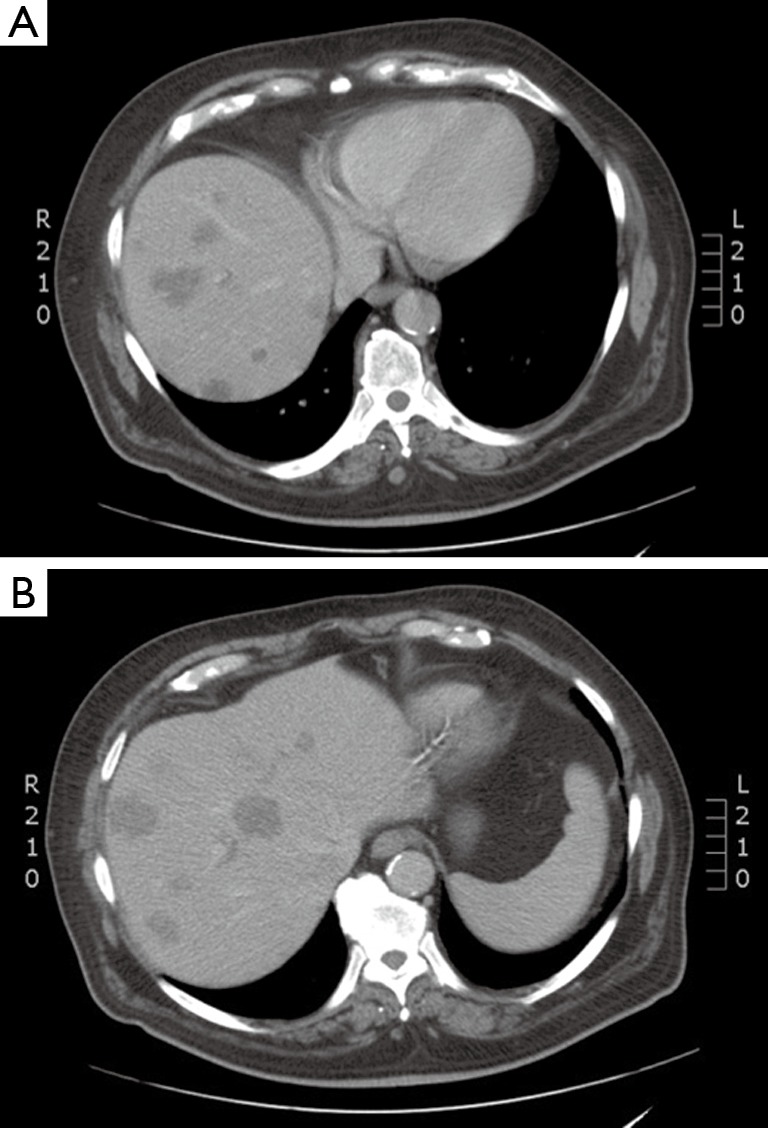
Pre and post-RFA appearance of colorectal hepatic metastasis. (A) Intra-procedural CT demonstrates RFA probe within left lobe hepatic metastasis; (B) post-procedure CT 6 months status post RFA demonstrates left lobe liver ablative lesion with no residual perfusion. RFA, radiofrequency ablation.
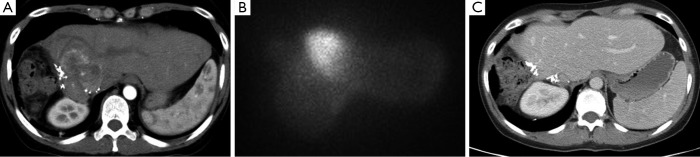
(A) Pre-radioembolization CT demonstrates enhancing colorectal hepatic metastasis; (B) immediate post-radioembolization bremsstrahlung scan demonstrates activity within the hepatic metastasis consistent with selective uptake of radioactive Y90 microspheres by the lesion; (C) 6-month post-treatment CT demonstrates complete response of the lesion.
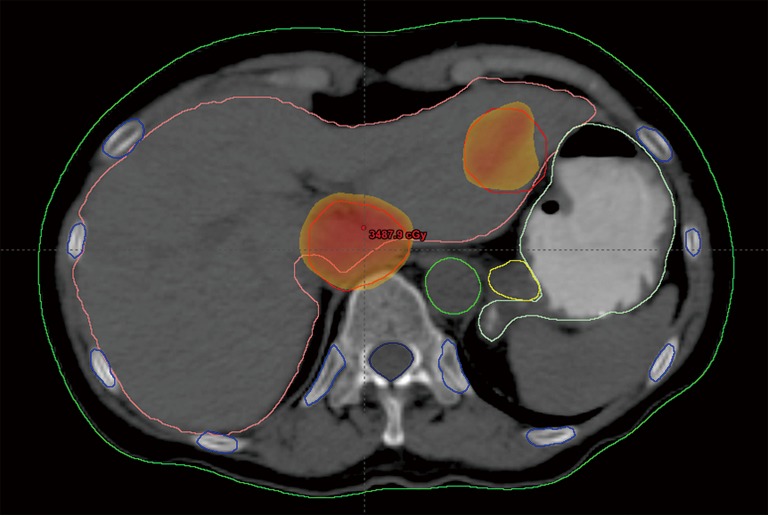
Two colorectal metastases at locations not amenable to RFA were treated with SBRT. RFA, radiofrequency ablation; SBRT, Stereotactic body radiotherapy.
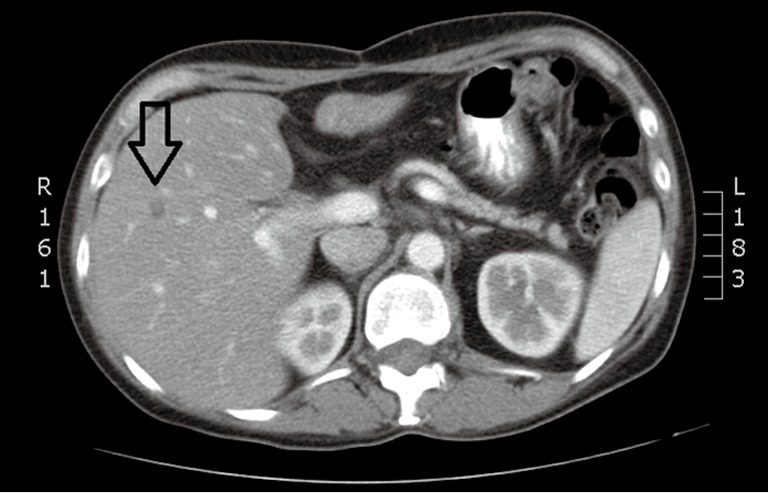
A solitary lesion in a non-surgical candidate, treated with RFA. RFA, radiofrequency ablation.
Diffuse liver metastases treated with radioembolization.
References
-
- Köhne CH, Lenz HJ. Chemotherapy with targeted agents for the treatment of metastatic colorectal cancer. Oncologist 2009;14:478-88. - PubMed
-
- Tabernero J, Van Cutsem E, Lakomý R, et al. Aflibercept versus placebo in combination with fluorouracil, leucovorin and irinotecan in the treatment of previously treated metastatic colorectal cancer: prespecified subgroup analyses from the VELOUR trial. Eur J Cancer 2014;50:320-31. - PubMed
-
- Peeters M, Price TJ, Cervantes A, et al. Final results from a randomized phase 3 study of FOLFIRI {+/-} panitumumab for second-line treatment of metastatic colorectal cancer. Ann Oncol 2014;25:107-16. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Medical