

Immunogenicity and safety of the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) co-administered with DTPa vaccine in Japanese children: A randomized, controlled study
- PMID: 25830489
- PMCID: PMC4514407
- DOI: 10.1080/21645515.2015.1012019
Immunogenicity and safety of the 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) co-administered with DTPa vaccine in Japanese children: A randomized, controlled study
Abstract
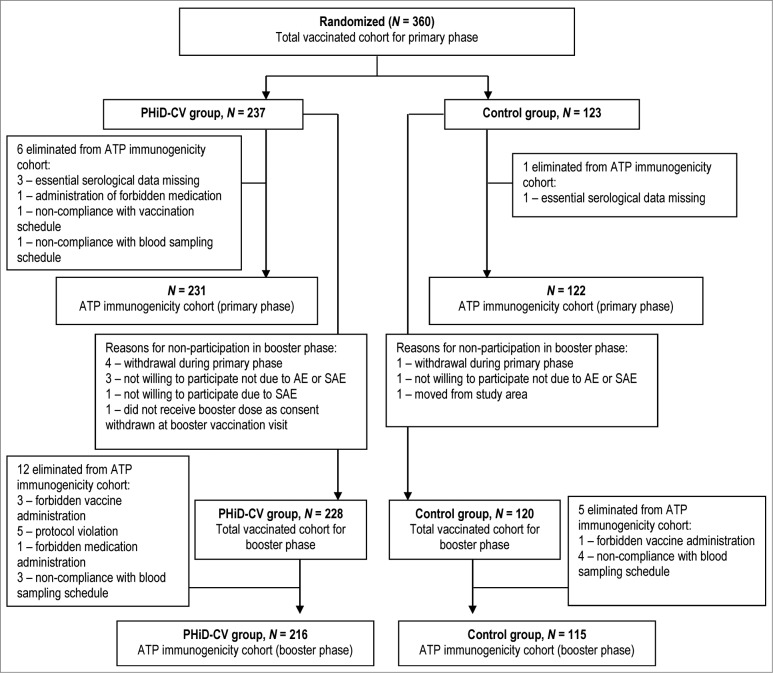
This phase III, randomized, open-label, multicenter study (NCT01027845) conducted in Japan assessed the immunogenicity, safety, and reactogenicity of 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV, given intramuscularly) co-administered with diphtheria-tetanus-acellular pertussis vaccine (DTPa, given subcutaneously). Infants (N=360 ) were randomized (2:1) to receive either PHiD-CV and DTPa (PHiD-CV group) or DTPa alone (control group) as 3-dose primary vaccination (3-4-5 months of age) and booster vaccination (17-19 months of age). Immune responses were measured before and one month after primary/booster vaccination and adverse events (AEs) were recorded. Post-primary immune responses were non-inferior to those in pivotal/efficacy European or Latin American pneumococcal protein D-conjugate vaccine studies. For each PHiD-CV serotype, at least 92.6% of infants post-primary vaccination and at least 97.7% of children post-booster had pneumococcal antibody concentrations ≥0.2 μg/ml, and at least 95.4% post-primary and at least 98.1% post-booster had opsonophagocytic activity (OPA) titers ≥8 . Geometric mean antibody concentrations and OPA titers (except OPA titer for 6B) were higher post-booster than post-priming for each serotype. All PHiD-CV-vaccinated children had anti-protein D antibody concentrations ≥100 EL.U/ml one month post-primary/booster vaccination and all were seroprotected/seropositive against each DTPa antigen. Redness and irritability were the most common solicited AEs in both groups. Incidences of unsolicited AEs were comparable between groups. Serious AEs were reported for 47 children (28 in PHiD-CV group); none were assessed as vaccine-related. In conclusion, PHiD-CV induced robust immune responses and was well tolerated when co-administered with DTPa in a 3-dose priming plus booster regimen to Japanese children.
Keywords: 7vCRM, 7-valent pneumococcal CRM-conjugate vaccine; AE, adverse event; AOM, acute otitis media; ATP, according-to-protocol; CAP, community-acquired pneumonia; CI, confidence interval; COMPAS, Clinical Otitis Media and PneumoniA Study; DTPa, diphtheria-tetanus-acellular pertussis; ELISA, enzyme-linked immunosorbent assay; GMC, geometric mean concentration; GMT, geometric mean titer; HBV, hepatitis B virus; Hib, Haemophilus influenzae type b; IPD, invasive pneumococcal disease; Japan; NTHi, nontypeable Haemophilus influenzae; OPA, opsonophagocytic activity; PCV, pneumococcal conjugate vaccine; PHiD-CV, 10-valent pneumococcal nontypeable Haemophilus influenzae protein D conjugate vaccine; POET, Pneumococcal Otitis Efficacy Trial; SAE, serious adverse event; SAS, Statistical Analysis System; SDD, SAS Drug and Development; WHO, World Health Organization; children; co-administration; immunogenicity; pneumococcal conjugate vaccine; safety.
Figures


Similar articles
-
Safety, reactogenicity and immunogenicity of 2-dose catch-up vaccination with 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) in Malian children in the second year of life: Results from an open study.Hum Vaccin Immunother. 2015;11(9):2207-14. doi: 10.1080/21645515.2015.1016679. Hum Vaccin Immunother. 2015. PMID: 26020101 Free PMC article. Clinical Trial.
-
Immunogenicity of the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) when coadministered with different neisseria meningitidis serogroup C conjugate vaccines.Pediatr Infect Dis J. 2009 Apr;28(4 Suppl):S77-88. doi: 10.1097/INF.0b013e318199f609. Pediatr Infect Dis J. 2009. PMID: 19325450 Clinical Trial.
-
Immunogenicity and safety of 10-valent pneumococcal non-typeable Haemophilus influenzae protein D-conjugate vaccine (PHiD-CV) co-administered with routine childhood vaccines in Taiwan.J Formos Med Assoc. 2012 Sep;111(9):495-503. doi: 10.1016/j.jfma.2011.07.014. Epub 2012 Mar 18. J Formos Med Assoc. 2012. PMID: 23021506 Clinical Trial.
-
Immunogenicity of routinely used childhood vaccines when coadministered with the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV).Pediatr Infect Dis J. 2009 Apr;28(4 Suppl):S97-S108. doi: 10.1097/INF.0b013e318199f61b. Pediatr Infect Dis J. 2009. PMID: 19325452 Review.
-
Safety and reactogenicity of the 10-valent pneumococcal non-typeable Haemophilus influenzae protein D conjugate vaccine (PHiD-CV) when coadministered with routine childhood vaccines.Pediatr Infect Dis J. 2009 Apr;28(4 Suppl):S109-18. doi: 10.1097/INF.0b013e318199f62d. Pediatr Infect Dis J. 2009. PMID: 19325447 Review.
Cited by
-
Revival of the heterologous prime-boost technique in COVID-19: An outlook from the history of outbreaks.Health Sci Rep. 2022 Feb 23;5(2):e531. doi: 10.1002/hsr2.531. eCollection 2022 Mar. Health Sci Rep. 2022. PMID: 35229055 Free PMC article. Review.
-
Panel 6: Vaccines.Otolaryngol Head Neck Surg. 2017 Apr;156(4_suppl):S76-S87. doi: 10.1177/0194599816632178. Otolaryngol Head Neck Surg. 2017. PMID: 28372533 Free PMC article. Review.
References
-
- O'Brien KL, Wolfson LJ, Watt JP, Henkle E, Deloria-Knoll M, McCall N, Lee E, Mulholland K, Levine OS, Cherian T. Burden of disease caused by Streptococcus pneumoniae in children younger than 5 years: global estimates. Lancet 2009; 374:893-902; PMID:19748398; http://dx.doi.org/10.1016/S0140-6736(09)61204-6 - DOI - PubMed
-
- Sakata H. Invasive Streptococcus pneumoniae infections in children in Kamikawa and Soya subprefecture, Hokkaido, Japan, 2000-2010, before the introduction of the 7-valent pneumococcal conjugate vaccine. J Infect Chemother 2011; 17:799-802; PMID:21701961; http://dx.doi.org/10.1007/s10156-011-0264-8 - DOI - PubMed
-
- Nakamura R, Togashi T. Population-based incidence of invasive Haemophilus influenzae and pneumococcal diseases before the introduction of vaccines in Japan. Pediatr Infect Dis J 2013; 32:1394-6; PMID:23804122; http://dx.doi.org/10.1097/INF.0b013e3182a14971 - DOI - PubMed
-
- Chiba N, Morozumi M, Sunaoshi K, Takahashi S, Takano M, Komori T, Sunakawa K, Ubukata K. Serotype and antibiotic resistance of isolates from patients with invasive pneumococcal disease in Japan. Epidemiol Infect 2010; 138:61-8; PMID:19538821; http://dx.doi.org/10.1017/S0950268809990239 - DOI - PubMed
-
- Sakai F, Chiba N, Ono A, Yamagata MS, Ubukata K, Sunakawa K, Takahashi T. Molecular epidemiologic characteristics of Streptococcus pneumoniae isolates from children with meningitis in Japan from 2007 through 2009. J Infect Chemother 2011; 17:334-40; PMID:21161561; http://dx.doi.org/10.1007/s10156-010-0180-3 - DOI - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous