

The volume ratio of ground glass opacity in early lung CT predicts mortality in acute paraquat poisoning
- PMID: 25830638
- PMCID: PMC4382148
- DOI: 10.1371/journal.pone.0121691
The volume ratio of ground glass opacity in early lung CT predicts mortality in acute paraquat poisoning
Abstract
Background: Pulmonary injury is the main cause of death in acute paraquat (PQ) poisoning. However, whether quantitative lung computed tomography (CT) can be useful in predicting the outcome of PQ poisoning remains unknown. We aimed to identify early findings of quantitative lung CT as predictors of outcome in acute PQ poisoning.
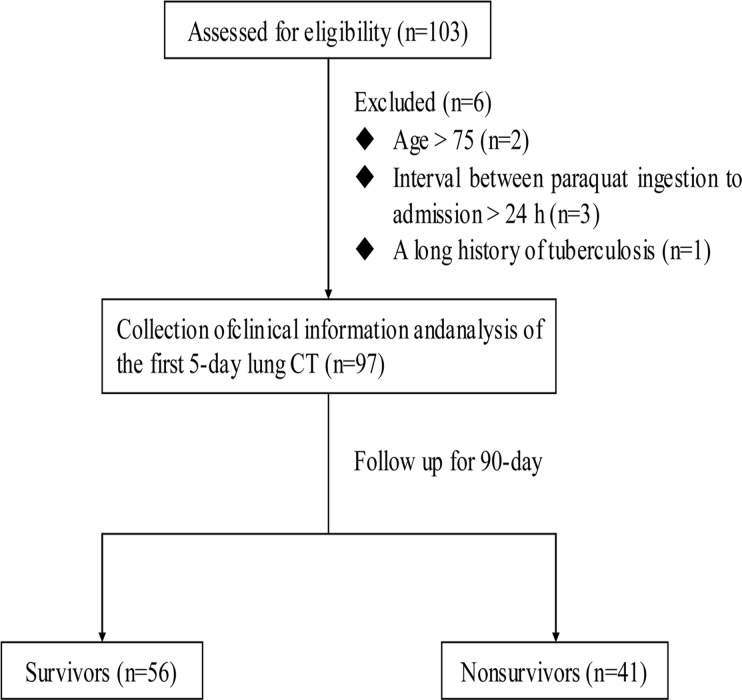
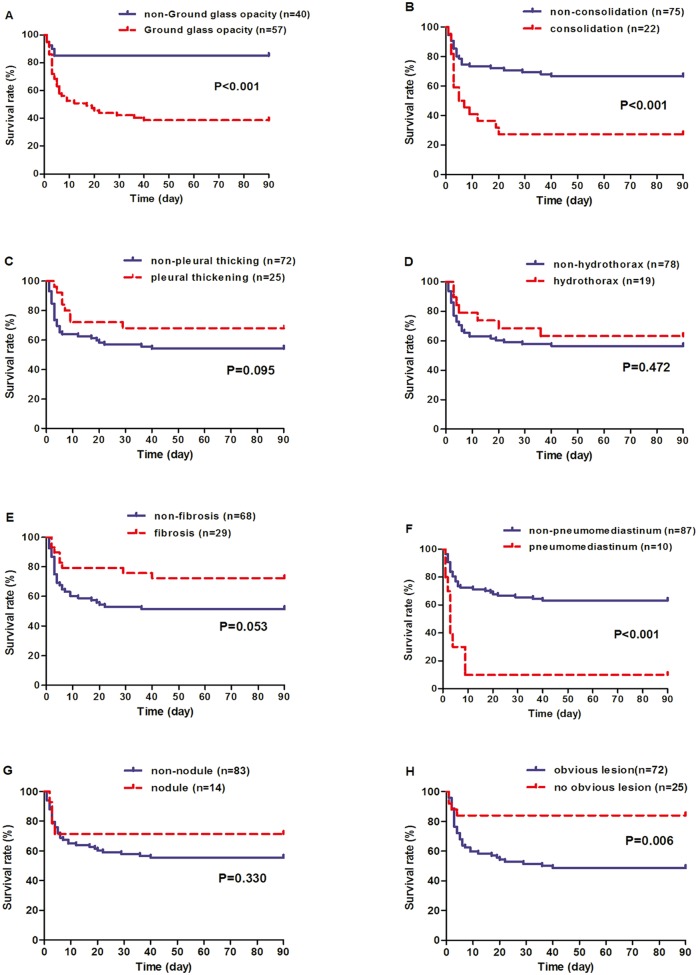
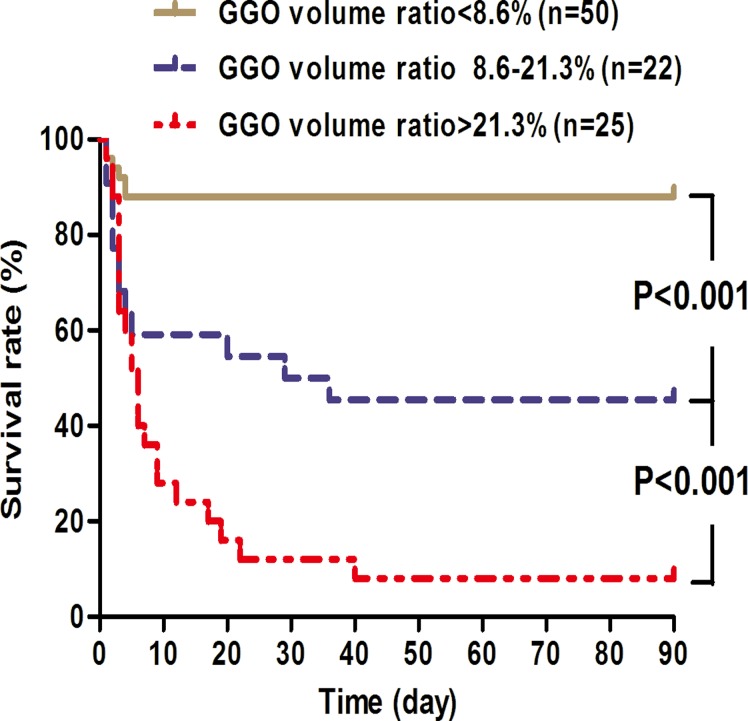
Methods: Lung CT scanning (64-slide) and quantitative CT lesions were prospectively measured for patients after PQ intoxication within 5 days. The study outcome was mortality during 90 days follow-up. Survival curves were derived by the Kaplan-Meier method, and mortality risk factors were analyzed by the forward stepwise Cox regression analysis.
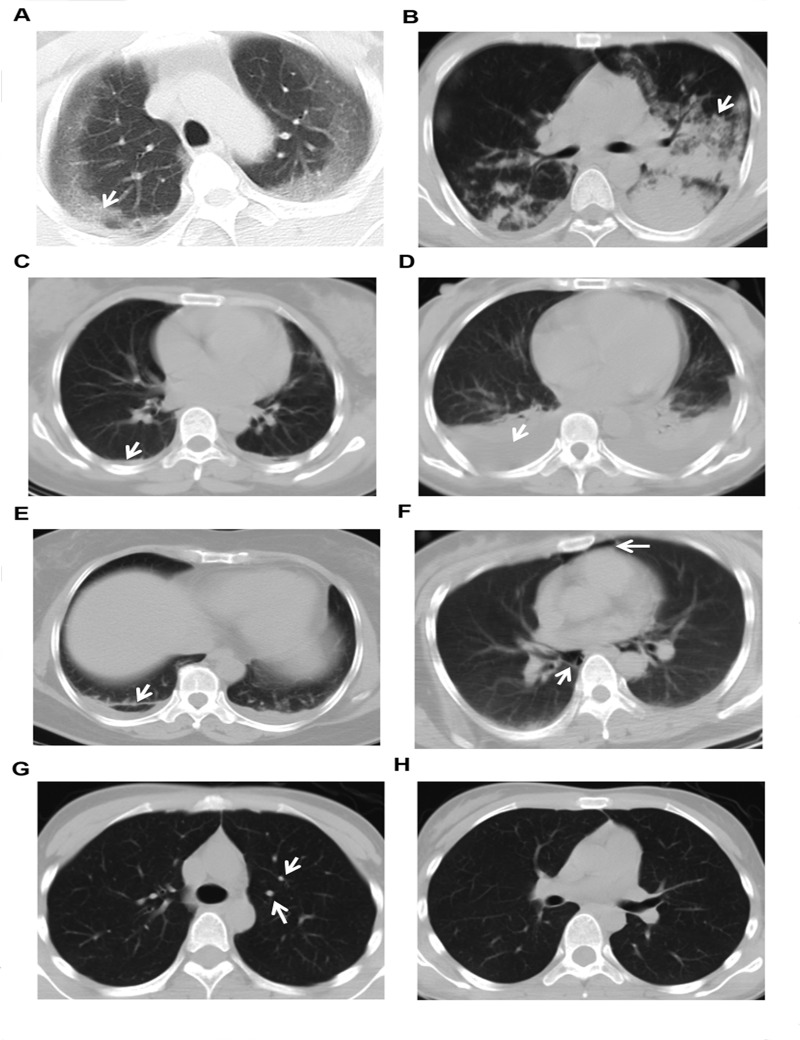
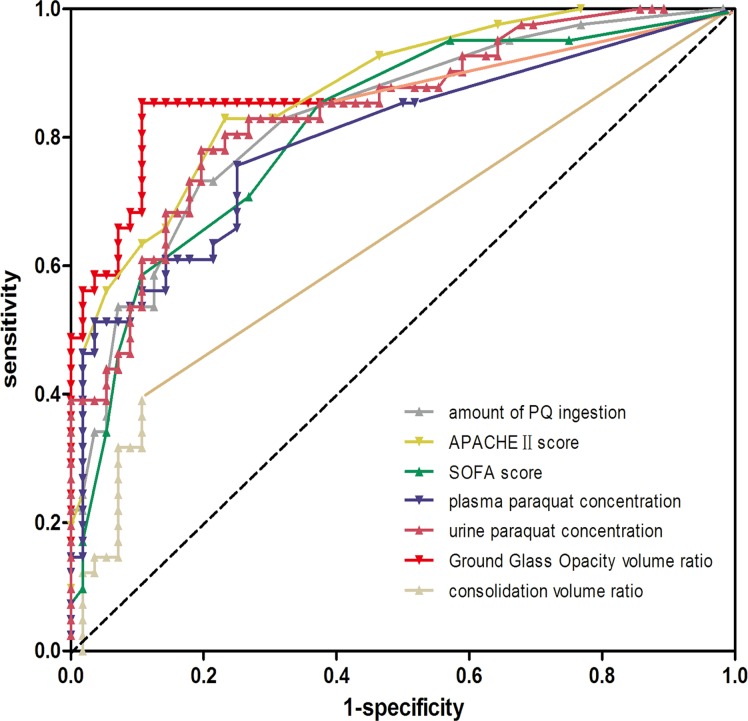
Results: Of 97 patients, 41 (42.3%) died. Among the eight different types of lung CT findings which appeared in the first 5-day of PQ intoxication, four ones discriminated between survivors and non-survivors including ground glass opacity (GGO), consolidation, pneumomediastinum and "no obvious lesion". With a cutoff value of 10.8%, sensitivity of 85.4% and specificity of 89.3%, GGO volume ratio is better than adopted outcome indicators in predicting mortality, such as estimated amount of PQ ingestion, plasma or urine PQ concentration, acute physiology and chronic health evaluation (APACHE) II and sequential organ failure assessment (SOFA) scores. GGO volume ratios above 10.8% were associated with increased mortality (hazard ratio, 5.82; 95% confidence interval, 4.77-7.09; P < 0.001).
Conclusions: The volume ratio of GGO exceeding 10.8% is a novel, reliable and independent predictors of outcome in acute PQ poisoning.
Conflict of interest statement
Figures
References
-
- Dinis-Oliveira RJ, Duarte JA, Sánchez-Navarro A, Remião F, Bastos ML, Carvalho F. (2008) Paraquat poisonings: mechanisms of lung toxicity, clinical features, and treatment. Crit Rev Toxicol 38: 13–71. - PubMed
-
- Lee EY, Hwang KY, Yang J-O, Hong SY. (2002) Predictors of survival after acute paraquat poisoning. Toxicol Ind Health 18: 201–206. - PubMed
-
- Proudfoot AT, Stewart MS, Levitt T, Widdop B. (1979) Paraquat poisoning: Significance of plasma-paraquat concentrations. Lancet 2: 330–332. - PubMed
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
