

High-intensity interval exercise and cerebrovascular health: curiosity, cause, and consequence
- PMID: 25833341
- PMCID: PMC4640257
- DOI: 10.1038/jcbfm.2015.49
High-intensity interval exercise and cerebrovascular health: curiosity, cause, and consequence
Abstract
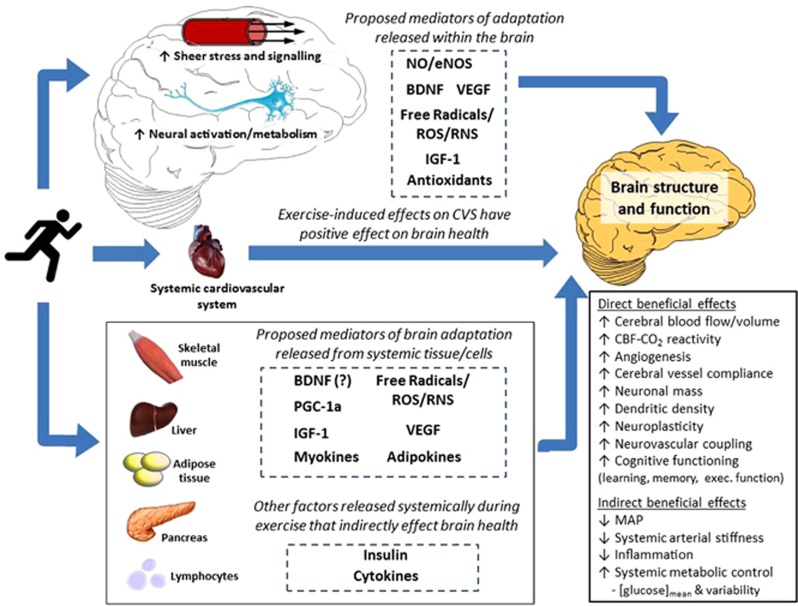
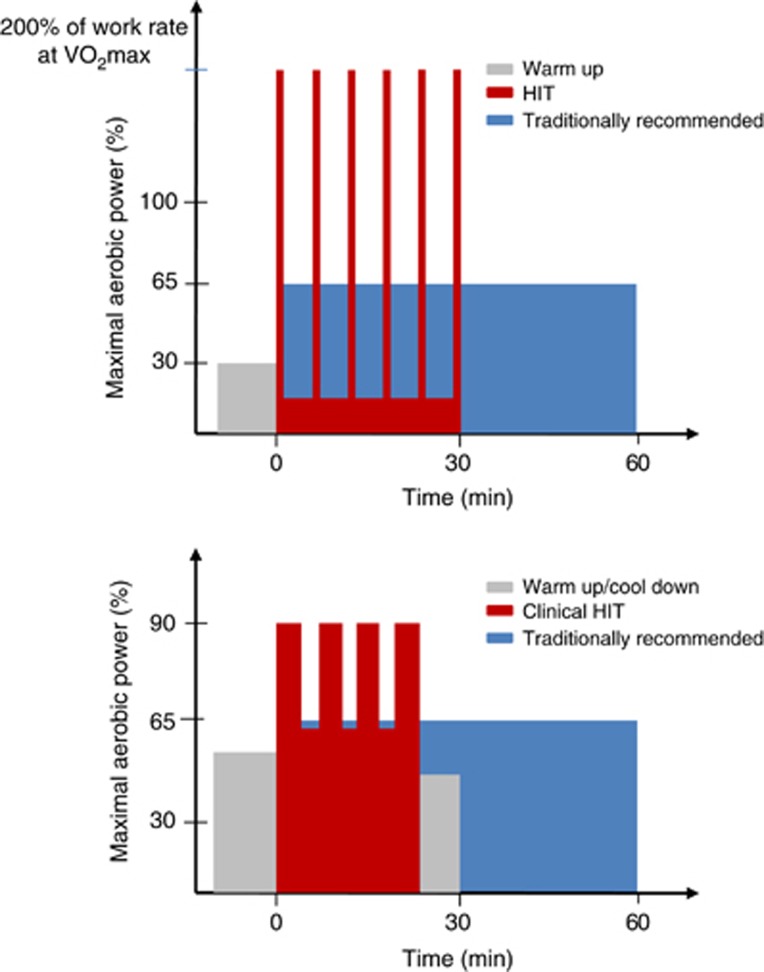
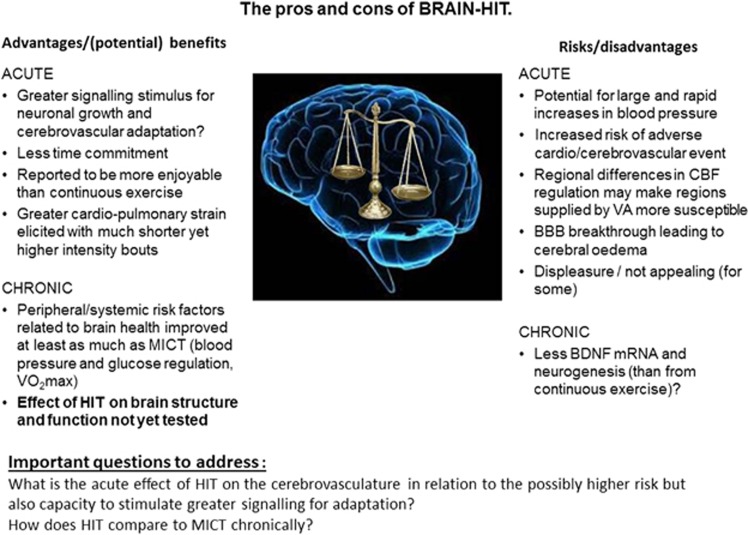
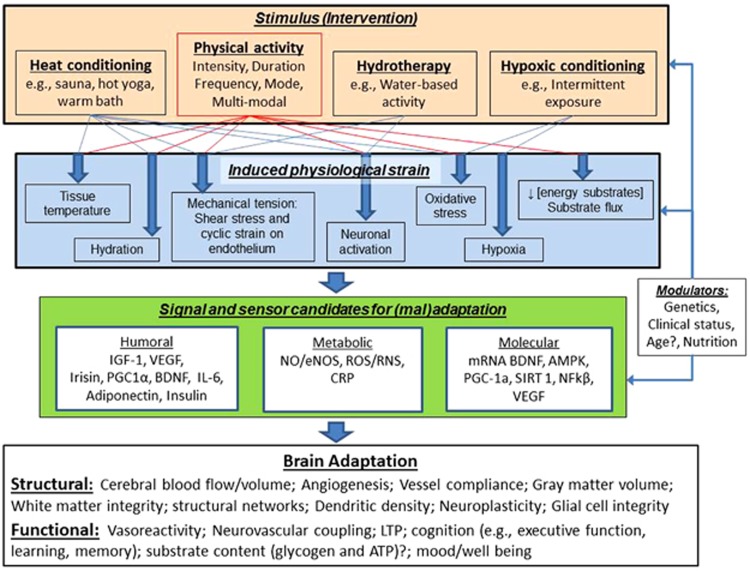
Exercise is a uniquely effective and pluripotent medicine against several noncommunicable diseases of westernised lifestyles, including protection against neurodegenerative disorders. High-intensity interval exercise training (HIT) is emerging as an effective alternative to current health-related exercise guidelines. Compared with traditional moderate-intensity continuous exercise training, HIT confers equivalent if not indeed superior metabolic, cardiac, and systemic vascular adaptation. Consequently, HIT is being promoted as a more time-efficient and practical approach to optimize health thereby reducing the burden of disease associated with physical inactivity. However, no studies to date have examined the impact of HIT on the cerebrovasculature and corresponding implications for cognitive function. This review critiques the implications of HIT for cerebrovascular function, with a focus on the mechanisms and translational impact for patient health and well-being. It also introduces similarly novel interventions currently under investigation as alternative means of accelerating exercise-induced cerebrovascular adaptation. We highlight a need for studies of the mechanisms and thereby also the optimal dose-response strategies to guide exercise prescription, and for studies to explore alternative approaches to optimize exercise outcomes in brain-related health and disease prevention. From a clinical perspective, interventions that selectively target the aging brain have the potential to prevent stroke and associated neurovascular diseases.
Figures
References
-
- 1Pedersen BK, Saltin B. Evidence for prescribing exercise as therapy in chronic disease. Scand J Med Sci Sports 2006; 16: 3–63. - PubMed
-
- 2Goldstein LB, Adams R, Alberts MJ, Appel LJ, Brass LM, Bushnell CD et al. Primary prevention of ischemic stroke: a guideline from the American Heart Association/American Stroke Association Stroke Council. Stroke 2006; 37: 1583–1633. - PubMed
-
- 3Lange-Asschenfeldt C, Kojda G. Alzheimer's disease, cerebrovascular dysfunction and the benefits of exercise: from vessels to neurons. Exp Gerontol 2008; 43: 499–504. - PubMed
-
- 4Stewart KJ, Hiatt WR, Regensteiner JG, Hirsch AT. Exercise training for claudication. New Engl J Med 2002; 347: 1941–1951. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
