

Minimally invasive decompression versus open laminectomy for central stenosis of the lumbar spine: pragmatic comparative effectiveness study
- PMID: 25833966
- PMCID: PMC4381635
- DOI: 10.1136/bmj.h1603
Minimally invasive decompression versus open laminectomy for central stenosis of the lumbar spine: pragmatic comparative effectiveness study
Abstract
Objective: To test the equivalence for clinical effectiveness between microdecompression and laminectomy in patients with central lumbar spinal stenosis.
Design: Multicentre observational study.
Setting: Prospective data from the Norwegian Registry for Spine Surgery.
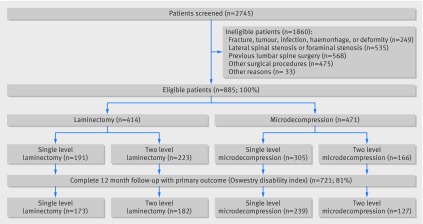
Participants: 885 patients with central stenosis of the lumbar spine who underwent surgery at 34 Norwegian orthopaedic or neurosurgical departments. Patients were treated from October 2006 to December 2011.
Interventions: Laminectomy and microdecompression.
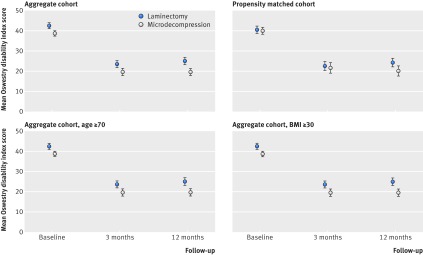
Main outcome measures: The primary outcome was change in Oswestry disability index score one year after surgery. Secondary endpoints were quality of life (EuroQol EQ-5D), perioperative complications, and duration of surgical procedures and hospital stays. A blinded biostatistician performed predefined statistical analyses in unmatched and propensity matched cohorts.
Results: The study was powered to detect a difference between the groups of eight points on the Oswestry disability index at one year. 721 patients (81%) completed the one year follow-up. Equivalence between microdecompression and laminectomy was shown for the Oswestry disability index (difference 1.3 points, 95% confidence interval -1.36 to 3.92, P<0.001 for equivalence). Equivalence was confirmed in the propensity matched cohort and full information regression analyses. No difference was found between groups in quality of life (EQ-5D) one year after surgery. The number of patients with complications was higher in the laminectomy group (15.0% v 9.8%, P=0.018), but after propensity matching for complications the groups did not differ (P=0.23). The duration of surgery for single level decompression was shorter in the microdecompression group (difference 11.2 minutes, 95% confidence interval 4.9 to 17.5, P<0.001), but after propensity matching the groups did not differ (P=0.15). Patients in the microdecompression group had shorter hospital stays, both for single level decompression (difference 1.5 days, 95% confidence interval 1.7 to 2.6, P<0.001) and two level decompression (0.8 days, 1.0 to 2.2, P=0.003).
Conclusion: At one year the effectiveness of microdecompression is equivalent to laminectomy in the surgical treatment of central stenosis of the lumbar spine. Favourable outcomes were observed at one year in both treatment groups.Trial registration ClinicalTrials.gov NCT02006901.
© Nerland et al 2015.
Conflict of interest statement
Competing interests: All authors have completed the ICMJE uniform disclosure form at
Figures
Comment in
-
Minimally invasive surgery for lumbar spinal stenosis.BMJ. 2015 Apr 1;350:h1664. doi: 10.1136/bmj.h1664. BMJ. 2015. PMID: 25832624 No abstract available.
References
-
- Katz JN, Harris MB. Clinical practice. Lumbar spinal stenosis. N Engl J Med 2008;358:818-25. - PubMed
-
- Amundsen T, Weber H, Nordal HJ, et al. Lumbar spinal stenosis: conservative or surgical management?: a prospective 10-year study. Spine (Phila Pa 1976) 2000;25:1424-35; discussion 1435-6. - PubMed
-
- Atlas SJ, Keller RB, Wu YA, et al. Long-term outcomes of surgical and nonsurgical management of lumbar spinal stenosis: 8 to 10 year results from the maine lumbar spine study. Spine (Phila Pa 1976) 2005;30:936-43. - PubMed
Publication types
MeSH terms
Associated data
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical