

Risk factors for failure of a single surgical debridement in adults with acute septic arthritis
- PMID: 25834080
- PMCID: PMC6948783
- DOI: 10.2106/JBJS.N.00593
Risk factors for failure of a single surgical debridement in adults with acute septic arthritis
Abstract
Background: Acute septic arthritis in a native joint may require more than one surgical debridement to eradicate the infection. Our objectives were to determine the prevalence of failure of a single surgical debridement for acute septic arthritis, to identify risk factors for failure of a single debridement, and to develop a prognostic probability algorithm to predict failure of a single surgical debridement for acute septic arthritis in adults.
Methods: We collected initial laboratory and medical comorbidity data of 128 adults (132 native joints) with acute septic arthritis who underwent at least one surgical debridement at our institution between 2000 and 2011. Univariate and logistic regression analyses were used to identify potential risk factors for failure of a single surgical debridement. Stepwise variable selection was used to develop a prediction model and identify probabilities of failure of a single surgical debridement.
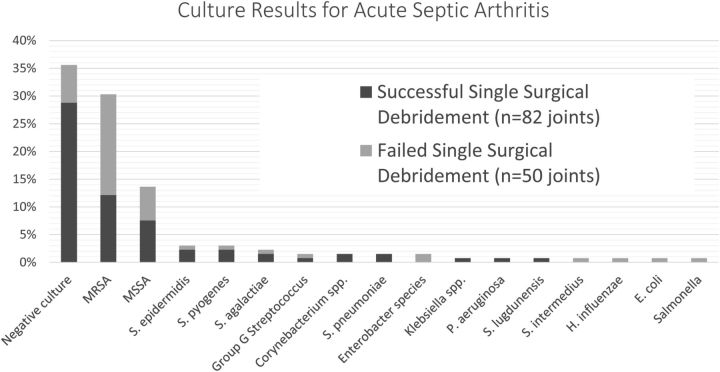
Results: Of the 128 patients (132 affected joints) who underwent surgical debridement for acute septic arthritis, forty-nine (38%) of the patients (fifty joints) experienced failure of a single debridement and required at least two debridements (range, two to four debridements). Staphylococcus aureus was the most common bacterial isolate (in sixty, or 45%, of the 132 joints). Logistic regression analysis identified five independent clinical predictors for failure of a single surgical debridement: a history of inflammatory arthropathy (odds ratio [OR], 7.3; 95% confidence interval [CI], 2.4 to 22.6; p < 0.001), the involvement of a large joint (knee, shoulder, or hip) (OR, 7.0; 95% CI, 1.2 to 37.5; p = 0.02), a synovial-fluid nucleated cell count of >85.0 x 10(9) cells/L (OR, 4.7; 95% CI, 1.8 to 17.7; p = 0.002), S. aureus as the bacterial isolate (OR, 4.6; 95% CI, 1.8 to 11.9; p = 0.002), and a history of diabetes (OR, 2.6; 95% CI, 1.1 to 6.2; p = 0.04).
Conclusions: Most (62%) of the septic joints were managed effectively with a single surgical debridement. Adults with a history of inflammatory arthropathy, involvement of a large joint, a synovial-fluid nucleated cell count of >85.0 x 10(9) cells/L, an infection with S. aureus, or a history of diabetes had a higher risk of failure of a single surgical debridement for acute septic arthritis and requiring additional surgical debridement(s).
Copyright © 2015 by The Journal of Bone and Joint Surgery, Incorporated.
Figures
References
-
- Chen CM, Lin HH, Hung SC, Huang TF, Chen WM, Liu CL, Chen TH. Surgical treatment for septic arthritis of the knee joint in elderly patients: a 10-year retrospective clinical study. Orthopedics. 2013. April;36(4):e434-43. - PubMed
-
- Riegels-Nielson P, Frimodt-Möller N, Jensen JS. Rabbit model of septic arthritis. Acta Orthop Scand. 1987. February;58(1):14-9. - PubMed
-
- Choi IH, Pizzutillo PD, Bowen JR, Dragann R, Malhis T. Sequelae and reconstruction after septic arthritis of the hip in infants. J Bone Joint Surg Am. 1990. September;72(8):1150-65. - PubMed
-
- Wada A, Fujii T, Takamura K, Yanagida H, Urano N, Surijamorn P. Operative reconstruction of the severe sequelae of infantile septic arthritis of the hip. J Pediatr Orthop. 2007. December;27(8):910-4. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
