

Neuregulin stimulation of cardiomyocyte regeneration in mice and human myocardium reveals a therapeutic window
- PMID: 25834111
- PMCID: PMC5360874
- DOI: 10.1126/scitranslmed.aaa5171
Neuregulin stimulation of cardiomyocyte regeneration in mice and human myocardium reveals a therapeutic window
Abstract
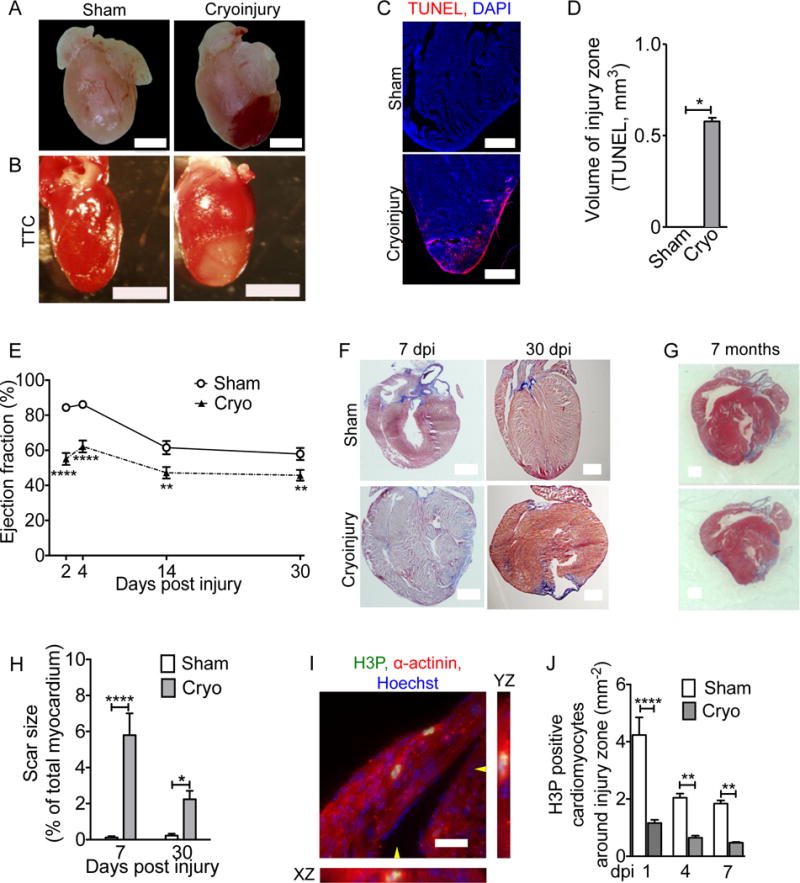
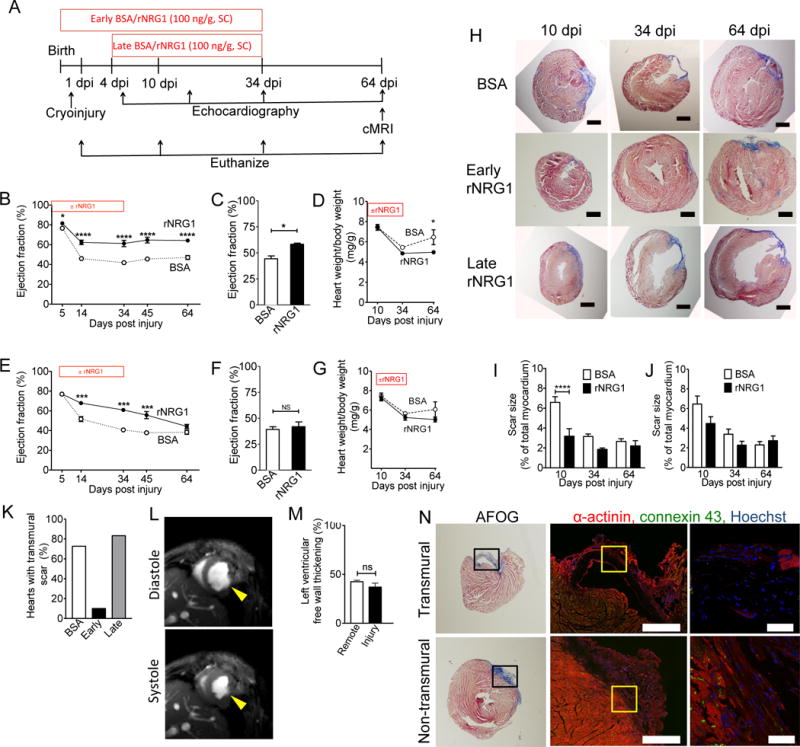
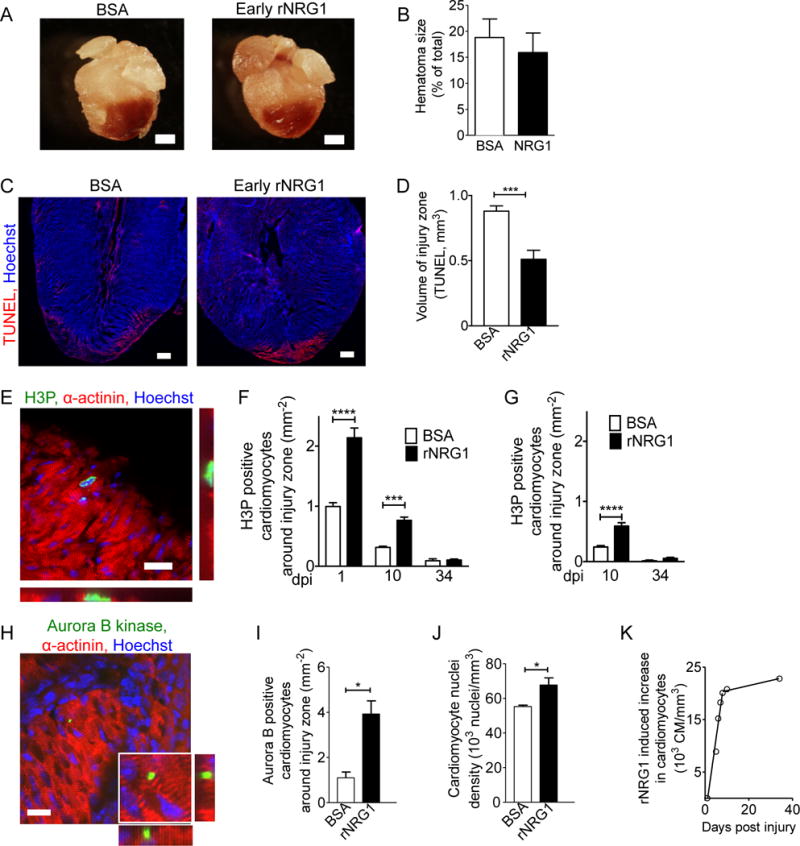
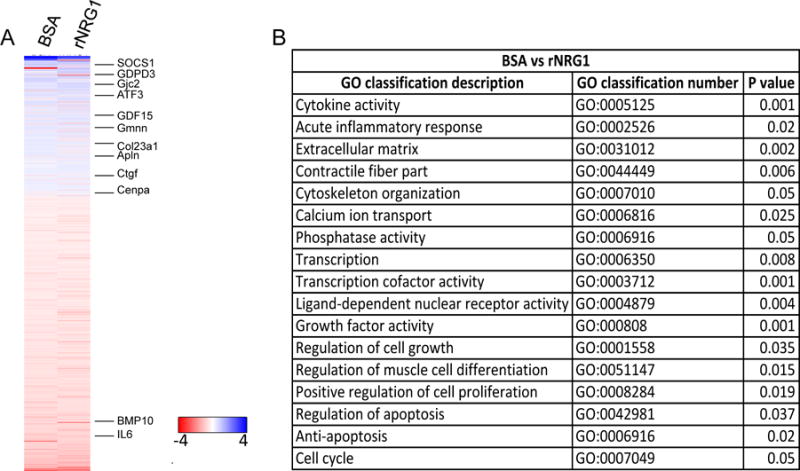
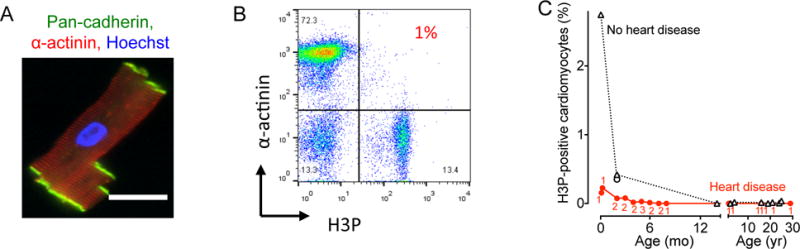
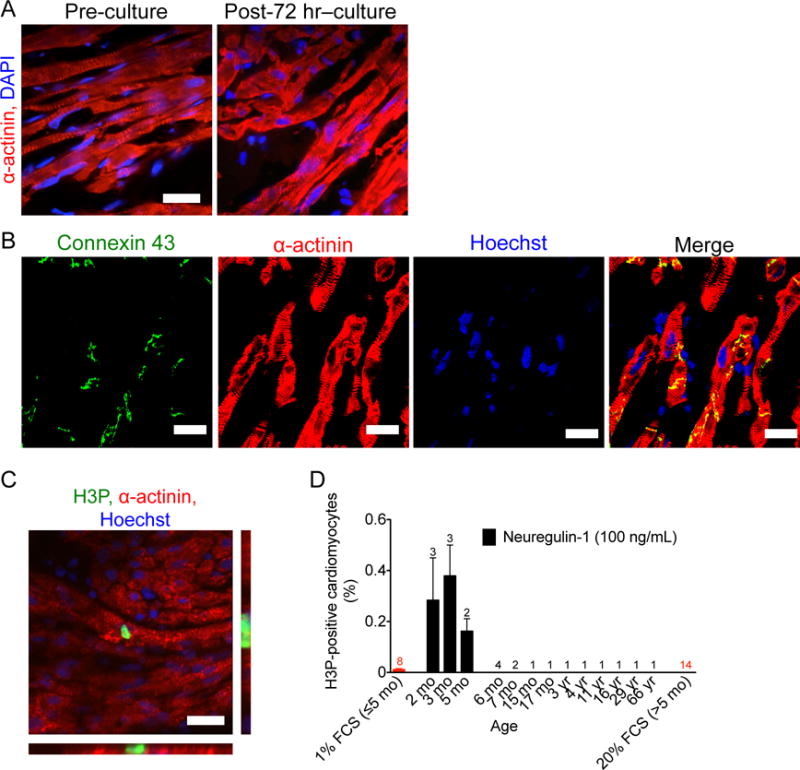
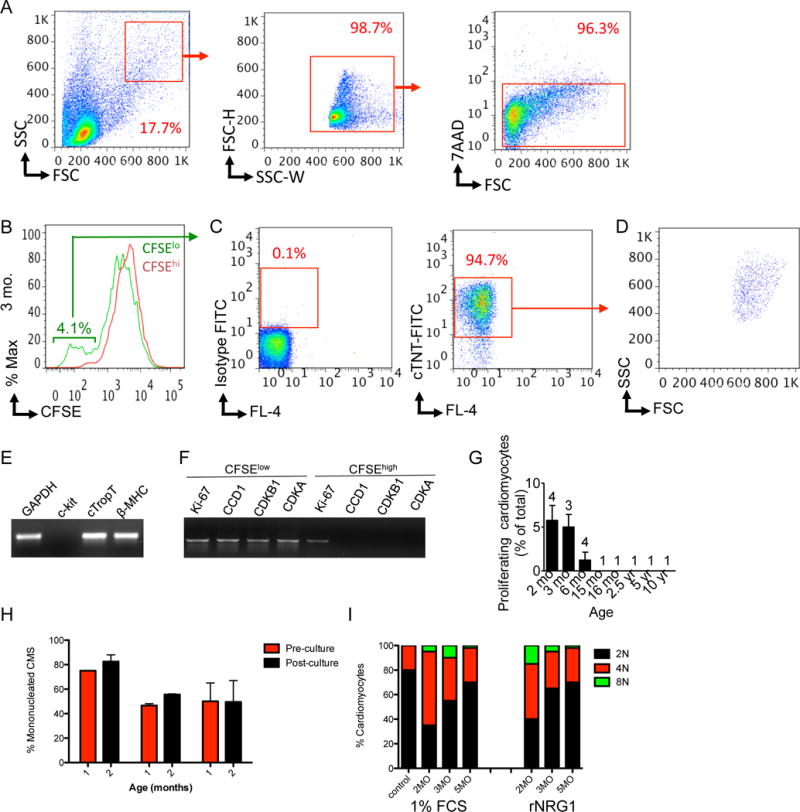
Therapies developed for adult patients with heart failure have been shown to be ineffective in pediatric clinical trials, leading to the recognition that new pediatric-specific therapies for heart failure must be developed. Administration of the recombinant growth factor neuregulin-1 (rNRG1) stimulates regeneration of heart muscle cells (cardiomyocytes) in adult mice. Because proliferation-competent cardiomyocytes are more abundant in growing mammals, we hypothesized that administration of rNRG1 during the neonatal period might be more effective than in adulthood. If so, neonatal rNRG1 delivery could be a new therapeutic strategy for treating heart failure in pediatric patients. To evaluate the effectiveness of rNRG1 administration in cardiac regeneration, newborn mice were subjected to cryoinjury, which induced myocardial dysfunction and scar formation and decreased cardiomyocyte cell cycle activity. Early administration of rNRG1 to mice from birth to 34 days of age improved myocardial function and reduced the prevalence of transmural scars. In contrast, administration of rNRG1 from 4 to 34 days of age only transiently improved myocardial function. The mechanisms of early administration involved cardiomyocyte protection (38%) and proliferation (62%). We also assessed the ability of rNRG1 to stimulate cardiomyocyte proliferation in intact cultured myocardium from pediatric patients. rNRG1 induced cardiomyocyte proliferation in myocardium from infants with heart disease who were less than 6 months of age. Our results identify an effective time period within which to execute rNRG1 clinical trials in pediatric patients for the stimulation of cardiomyocyte regeneration.
Copyright © 2015, American Association for the Advancement of Science.
Conflict of interest statement
Figures

References
-
- Tennant PW, Pearce MS, Bythell M, Rankin J. 20-year survival of children born with congenital anomalies: a population-based study. Lancet. 2010;375:649. - PubMed
-
- Hoffman JI, Kaplan S. The incidence of congenital heart disease. J Am Coll Cardiol. 2002;39:1890. - PubMed
-
- Bolger AP, Coats AJ, Gatzoulis MA. Congenital heart disease: the original heart failure syndrome. Eur Heart J. 2003;24:970. - PubMed
-
- Burns KM, Byrne BJ, Gelb BD, Kuhn B, Leinwand LA, Mital S, Pearson GD, Rodefeld M, Rossano JW, Stauffer BL, Taylor MD, Towbin JA, Redington AN. New mechanistic and therapeutic targets for pediatric heart failure: report from a National Heart, Lung, and Blood Institute Working Group. Circulation. 2014;130:79. - PMC - PubMed
-
- Shaddy RE, Boucek MM, Hsu DT, Boucek RJ, Canter CE, Mahony L, Ross RD, Pahl E, Blume ED, Dodd DA, Rosenthal DN, Burr J, LaSalle B, Holubkov R, Lukas MA, Tani LY. Carvedilol for children and adolescents with heart failure: a randomized controlled trial. JAMA: the journal of the American Medical Association. 2007;298:1171. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Molecular Biology Databases
