Ultrasonography-guided surgical clip placement for tumor localization in patients undergoing neoadjuvant chemotherapy for breast cancer
- PMID: 25834610
- PMCID: PMC4381122
- DOI: 10.4048/jbc.2015.18.1.44
Ultrasonography-guided surgical clip placement for tumor localization in patients undergoing neoadjuvant chemotherapy for breast cancer
Abstract
Purpose: We investigated the feasibility of using surgical clips as markers for tumor localization and their effect on the imaging evaluation of treatment responses after neoadjuvant chemotherapy (NAC).
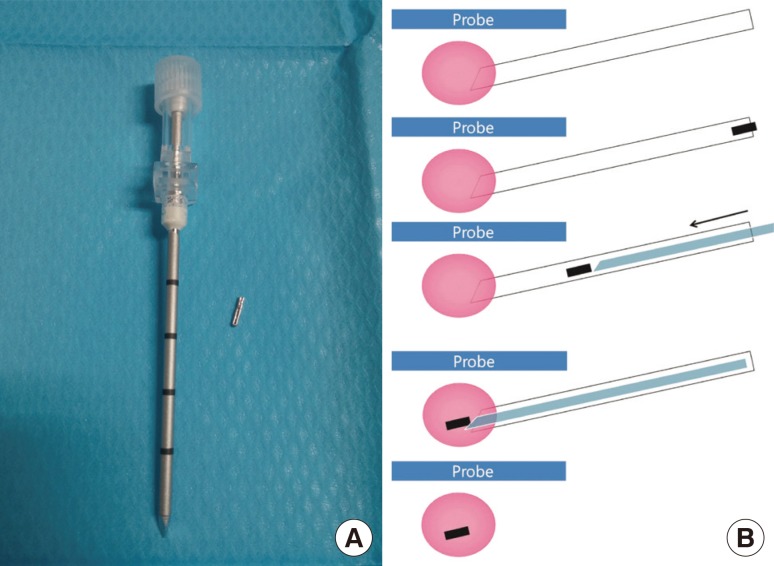
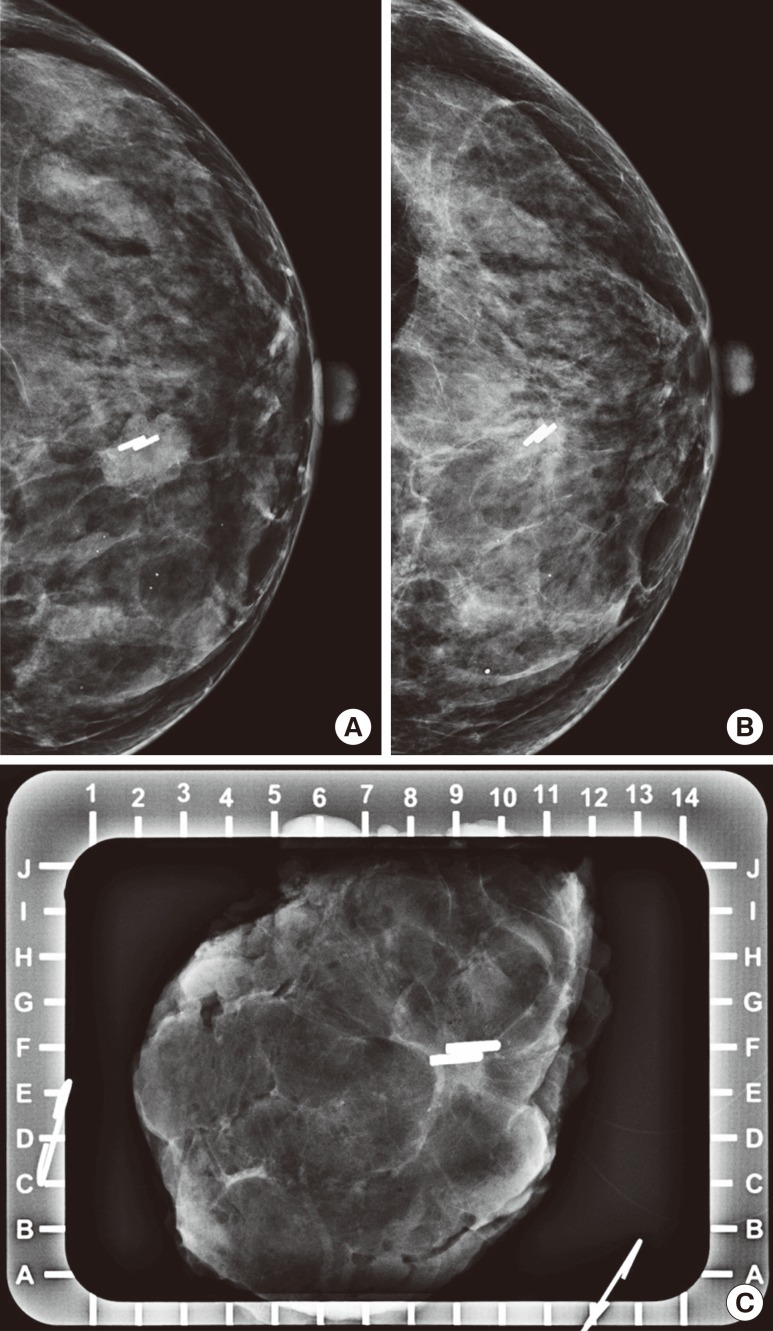
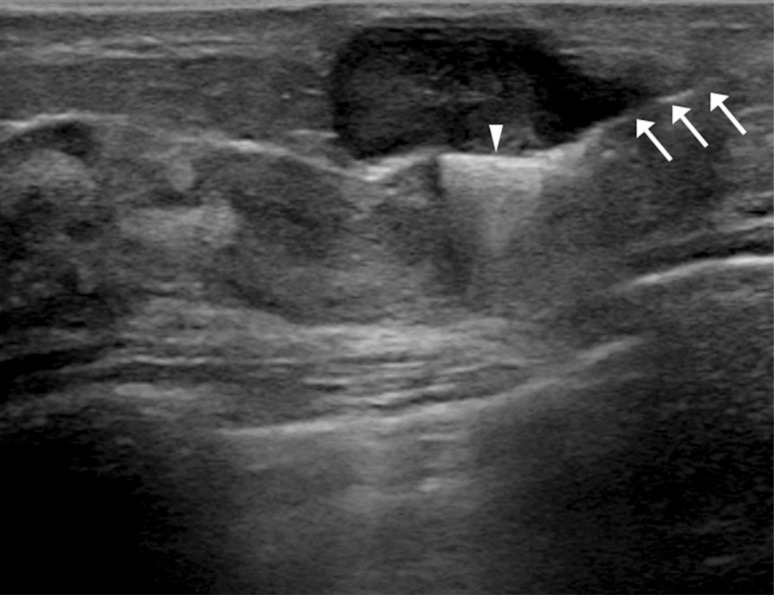
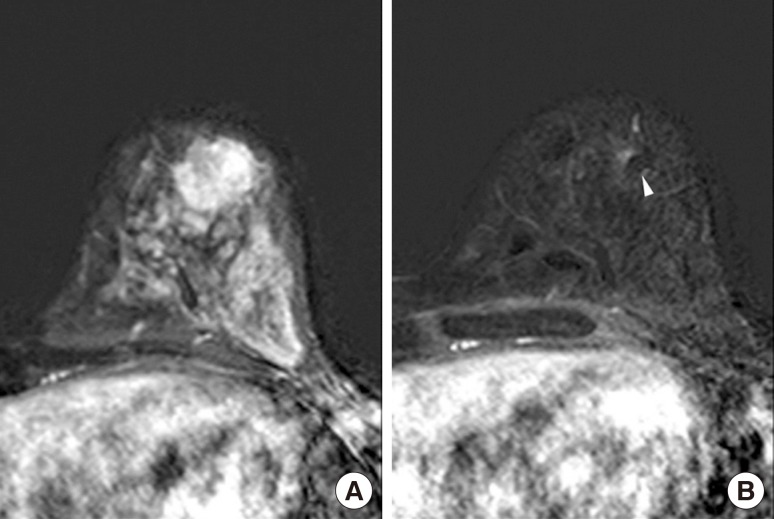
Methods: A total of 16 breast cancers confirmed by needle biopsy in 15 patients were included in this study from October 2012 to June 2014. Under ultrasonography (US)-guidance, the surgical clips were placed prior to NAC. Additional mammography, breast US, and breast magnetic resonance examinations were performed within 10 days before surgery. The time period from marker insertion to operation date was documented. Images acquired via the three modalities were evalu-ated for the following parameters: location of clip, clip migration (>1 cm), the presence of complications from clip placement, and the effect of clips on the assessment of treatment.
Results: The mean time period was 128.6±34.4 days (median, 132.0 days) from the date of clip insertion to the date of surgery. The mean number of inserted clips was 2.3±0.7 (median, 2.0). Clip migration was not visualized by imaging in any patient, and there were no complications reported. Surgical clips did not negatively affect the assessment of treatment responses to NAC.
Conclusion: Surgical clips may replace commercial tissue markers for tumor localization in breast cancer patients undergoing NAC without migration. Surgical clips are well tolerated and safe for the patient, easily visualized on imaging, do not interfere with treatment response, and are cost-effective.
Keywords: Breast neoplasms; Image-guided biopsy; Neoadjuvant therapy; Surgical instruments; Ultrasonography.
Conflict of interest statement
Figures
References
-
- Kaufmann M, von Minckwitz G, Bear HD, Buzdar A, McGale P, Bonnefoi H, et al. Recommendations from an international expert panel on the use of neoadjuvant (primary) systemic treatment of operable breast cancer: new perspectives 2006. Ann Oncol. 2007;18:1927–1934. - PubMed
-
- Lobbes MB, Prevos R, Smidt M, Tjan-Heijnen VC, van Goethem M, Schipper R, et al. The role of magnetic resonance imaging in assessing residual disease and pathologic complete response in breast cancer patients receiving neoadjuvant chemotherapy: a systematic review. Insights Imaging. 2013;4:163–175. - PMC - PubMed
LinkOut - more resources
Full Text Sources
Other Literature Sources