

Headache in pregnancy: an approach to emergency department evaluation and management
- PMID: 25834672
- PMCID: PMC4380381
- DOI: 10.5811/westjem.2015.1.23688
Headache in pregnancy: an approach to emergency department evaluation and management
Abstract
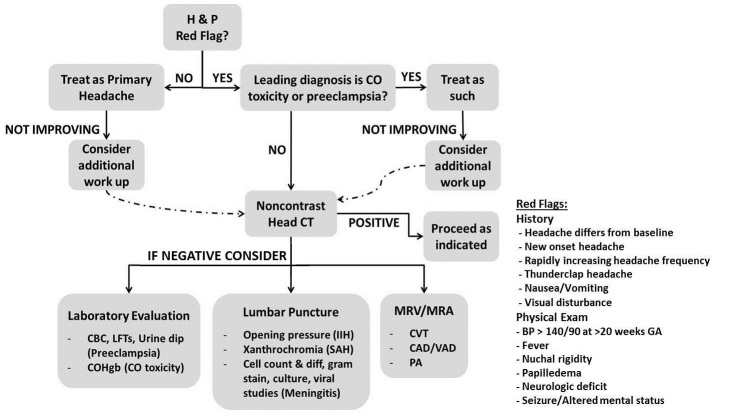
Headache is a common presenting complaint in the emergency department. The differential diagnosis is broad and includes benign primary causes as well as ominous secondary causes. The diagnosis and management of headache in the pregnant patient presents several challenges. There are important unique considerations regarding the differential diagnosis, imaging options, and medical management. Physiologic changes induced by pregnancy increase the risk of cerebral venous thrombosis, dissection, and pituitary apoplexy. Preeclampsia, a serious condition unique to pregnancy, must also be considered. A high index of suspicion for carbon monoxide toxicity should be maintained. Primary headaches should be a diagnosis of exclusion. When advanced imaging is indicated, magnetic resonance imaging (MRI) should be used, if available, to reduce radiation exposure. Contrast agents should be avoided unless absolutely necessary. Medical therapy should be selected with careful consideration of adverse fetal effects. Herein, we present a review of the literature and discuss an approach to the evaluation and management of headache in pregnancy.
Figures
References
-
- Backes D, Rinkel GJE, Kemperman H, et al. Time-dependent test characteristics of head computed tomography in patients suspected of nontraumatic subarachnoid hemorrhage. Stroke. 2012;43:2115–19. - PubMed
-
- Edlow JA, Caplan LR. Avoiding pitfalls in the diagnosis of subarachnoid hemorrhage. N Engl J Med. 2000;342:29–36. - PubMed
-
- Edlow JA, Bruner KS, Horowitz GL. Xanthochromia: A survey of laboratory methodology and its clinical implications. Arch Pathol Lab Med. 2002;126:413–15. - PubMed
-
- Guidelines for diagnostic imaging during pregnancy. ACOG Committee Opinion #299. American College of Obstetricians and Gynecologists. Obstet Gynecol. 2004;104:647–51. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
