

Critical Review: Building on the HIV Cascade: A Complementary "HIV States and Transitions" Framework for Describing HIV Diagnosis, Care, and Treatment at the Population Level
- PMID: 25835604
- PMCID: PMC4506700
- DOI: 10.1097/QAI.0000000000000611
Critical Review: Building on the HIV Cascade: A Complementary "HIV States and Transitions" Framework for Describing HIV Diagnosis, Care, and Treatment at the Population Level
Abstract
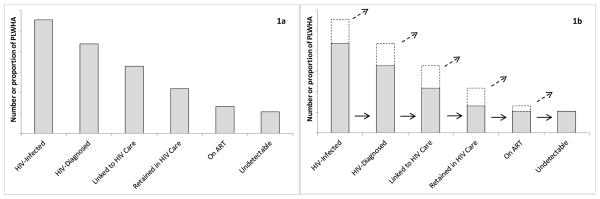
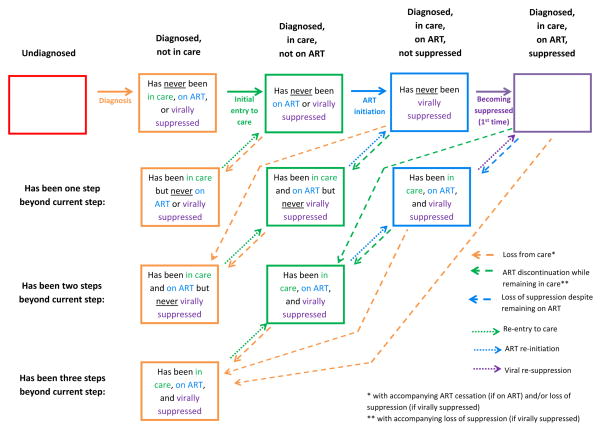
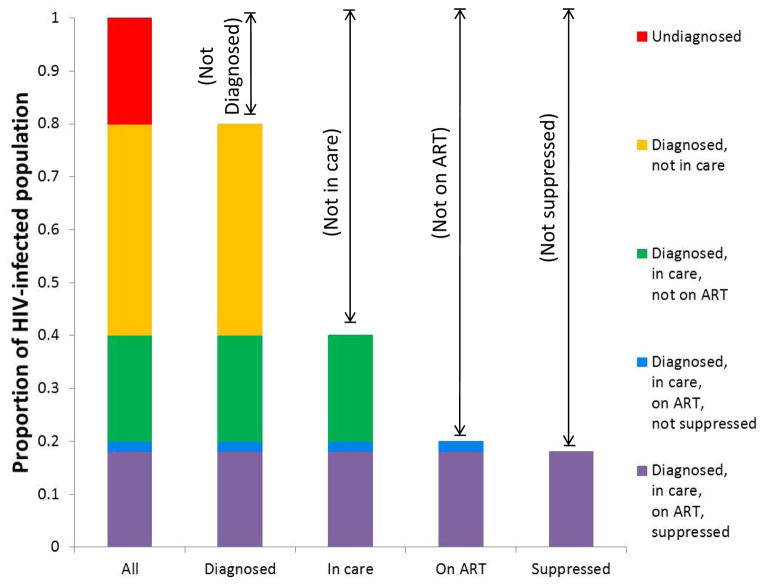
The HIV cascade--often referred to as "the HIV continuum"--provides a valuable framework for population-level representations of engagement with the HIV healthcare system. The importance and appeal of this framework are evidenced by a large body of scientific literature, as well as by the adoption of cascade-related indicators by medical and public health organizations worldwide. Despite its centrality in the fields of HIV treatment and prevention, however, the traditional cascade provides limited description of the processes affecting the numbers it represents. Representations that describe these processes and capture the dynamic nature of HIV-infected persons' pathways through the healthcare system are essential for monitoring and predicting intervention effects and epidemic trends. We propose here a complementary schema--termed the "HIV States and Transitions" framework--designed to maintain key strengths of the traditional cascade while addressing key limitations and more fully describing the dynamic aspects of HIV testing, care, and treatment at the population level.
Conflict of interest statement
Figures
References
-
- Greenberg AE, Hader SL, Masur H, et al. Fighting HIV/AIDS in Washington, DC. Health Aff. 2009;28:1677–1687. - PubMed
-
- Cohen S, Van Handel MM, Branson BM, et al. Vital Signs: HIV prevention through care and treatment. MMWR. 2011;60:1618–1623. - PubMed
-
- World Health Organization. Consolidated guidelines on the use of antiretroviral drugs for treating and preventing HIV infection. Geneva: World Health Organization; 2013. [Accessed 13 June 2014]. Available at: http://www.who.int/hiv/pub/guidelines/arv2013/en/
-
- Office of National AIDS Policy (US) National HIV/AIDS strategy for the United States. Washington: Office of National AIDS Policy; 2010. [Accessed 13 June 2014]. Available at: http://www.whitehouse.gov/sites/default/files/uploads/NHAS.pdf.
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Medical
