

Disparities in cardiovascular research output and citations from 52 African countries: a time-trend, bibliometric analysis (1999-2008)
- PMID: 25836056
- PMCID: PMC4579930
- DOI: 10.1161/JAHA.114.001606
Disparities in cardiovascular research output and citations from 52 African countries: a time-trend, bibliometric analysis (1999-2008)
Abstract
Background: Cardiovascular research output and citations of publications from Africa have historically been low yet may be increasing. However, data from the continent are limited.
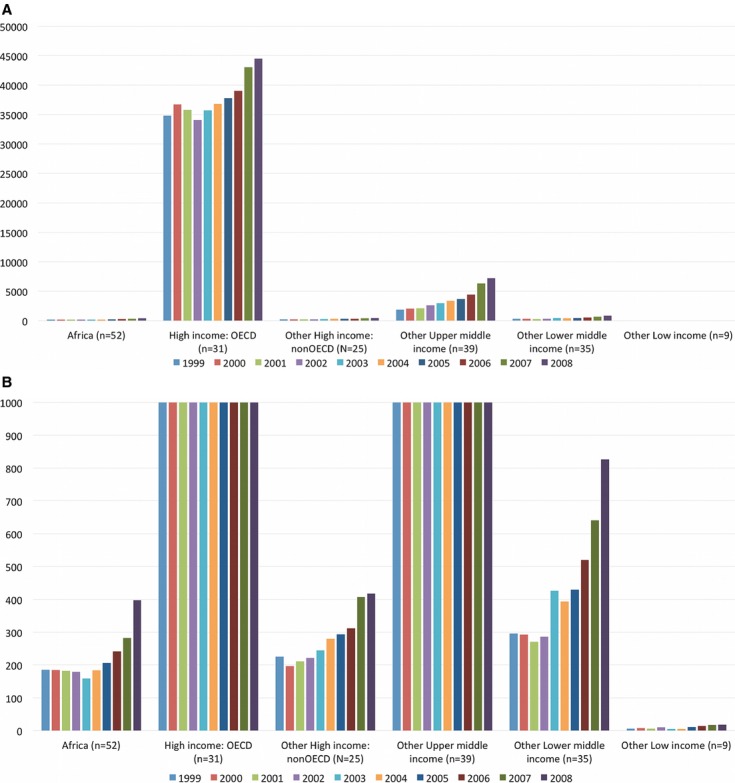
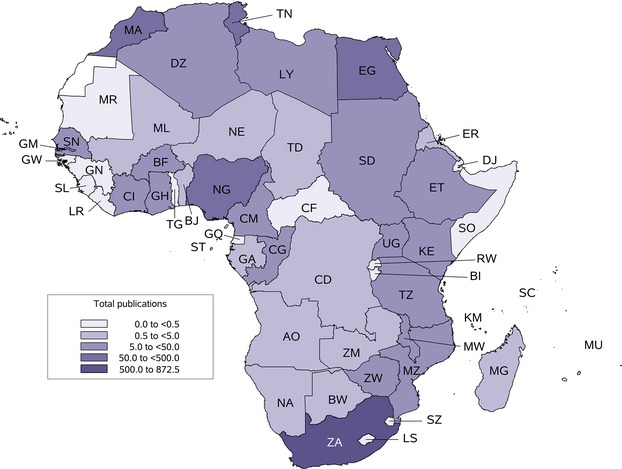
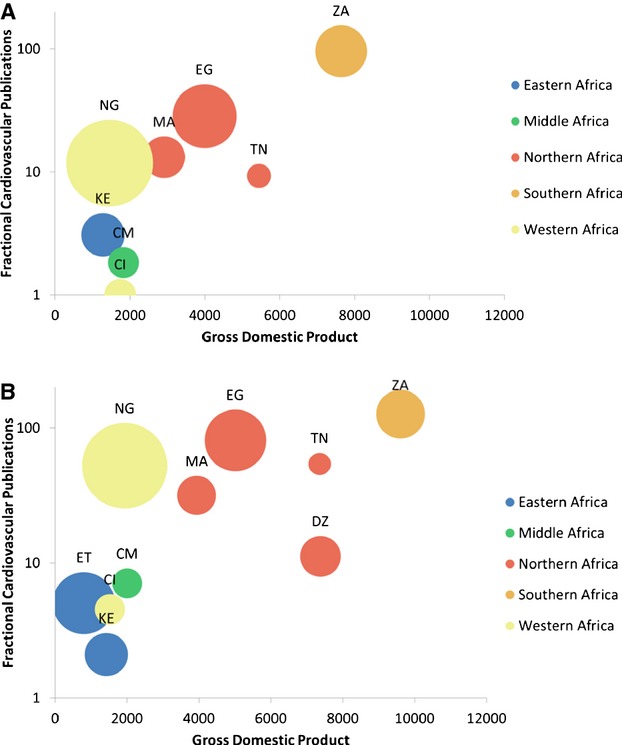
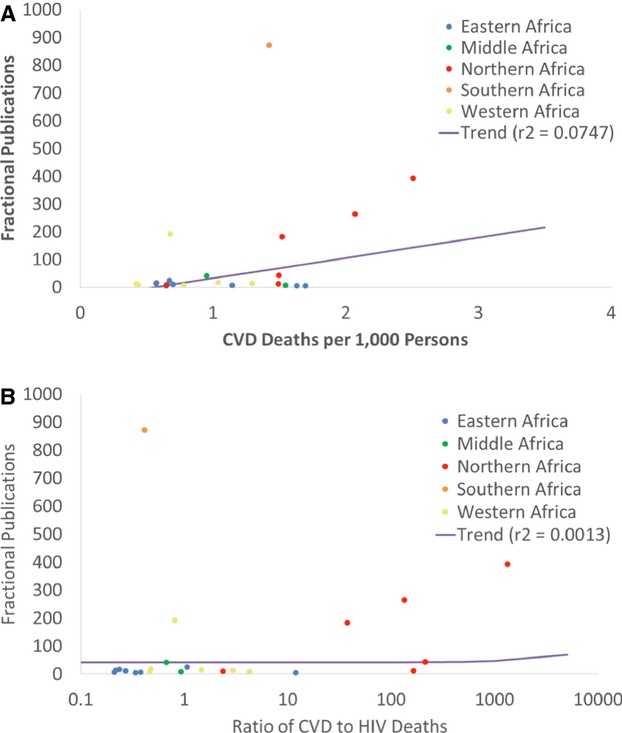
Methods and results: To evaluate the cardiovascular research output and citations from 52 African countries between 1999 and 2008, we created a bibliometric filter to capture cardiovascular research articles published in the Web of Knowledge based on specialist journals and title words. Two coauthors with expertise in cardiovascular medicine tested and refined this filter to achieve >90% precision and recall. We matched retrieved records with their associated citation reports and calculated the running 5-year citation count postpublication, including the year of publication. Publications from Africa were identified by author addresses. South Africa published 872 cardiovascular research papers, Egypt 393, Tunisia 264, and Nigeria 192 between 1999 and 2008. The number of publications increased over the time period for a small number of countries (range 0.1 to 4.8 more publications per year by fractional count). Most countries' citations were low (<50), but citations were greatest for South Africa (7063), Egypt (2557), Tunisia (903), and Nigeria (540). The same countries had the greatest annual increase in 5-year citation index values: 65 (95% CI: 30, 99) for South Africa, 46 (34, 58) for Egypt, 22 (15, 28) for Tunisia, and 8 (2, 14) for Nigeria. The burden of cardiovascular disease had a weak and inconsistent relationship to cardiovascular publications (r(2)=0.07, P=0.05). Greater gross domestic product was associated with more cardiovascular publications in 2008 (r(2)=0.53, P<0.0001).
Conclusions: The increases in cardiovascular research outputs from Africa are concentrated in a few countries. The reasons for regional differences in research outputs require further investigation, particularly relative to competing disease burdens. Higher prioritization of cardiovascular research funding from African countries is warranted.
Keywords: cardiovascular diseases; publications; research; trends.
© 2015 The Authors. Published on behalf of the American Heart Association, Inc., by Wiley Blackwell.
Figures
Similar articles
-
Bibliometric analysis of literature on female genital mutilation: (1930 - 2015).Reprod Health. 2016 Oct 10;13(1):130. doi: 10.1186/s12978-016-0243-8. Reprod Health. 2016. PMID: 27724920 Free PMC article.
-
Cardiovascular research publications from Latin America between 1999 and 2008. A bibliometric study.Arq Bras Cardiol. 2015 Jan;104(1):5-15. doi: 10.5935/abc.20140213. Arq Bras Cardiol. 2015. PMID: 25714407 Free PMC article.
-
Global cardiovascular research output, citations, and collaborations: a time-trend, bibliometric analysis (1999-2008).PLoS One. 2013 Dec 31;8(12):e83440. doi: 10.1371/journal.pone.0083440. eCollection 2013. PLoS One. 2013. PMID: 24391769 Free PMC article.
-
China's Contribution to Anesthesiology Research: A 10-Year Survey of the Literature.Anesth Analg. 2016 May;122(5):1640-5. doi: 10.1213/ANE.0000000000001225. Anesth Analg. 2016. PMID: 27003916 Review.
-
Footprint and imprint: an ecologic time-trend analysis of cardiovascular publications in general and specialty journals.Glob Heart. 2014 Jun;9(2):263-269.e2. doi: 10.1016/j.gheart.2013.12.006. Glob Heart. 2014. PMID: 25667098 Review.
Cited by
-
Knowledge domain and emerging trends in post-stroke cognitive impairment: a bibliometric analysis.Front Aging Neurosci. 2025 Mar 4;17:1525626. doi: 10.3389/fnagi.2025.1525626. eCollection 2025. Front Aging Neurosci. 2025. PMID: 40103932 Free PMC article.
-
Disparities in Cardiovascular Research Output and Disease Outcomes among High-, Middle- and Low-Income Countries - An Analysis of Global Cardiovascular Publications over the Last Decade (2008-2017).Glob Heart. 2021 Jan 18;16(1):4. doi: 10.5334/gh.815. Glob Heart. 2021. PMID: 33598384 Free PMC article.
-
Resource Effective Strategies to Prevent and Treat Cardiovascular Disease.Circulation. 2016 Feb 23;133(8):742-55. doi: 10.1161/CIRCULATIONAHA.115.008721. Circulation. 2016. PMID: 26903017 Free PMC article. Review.
-
Markers of Atherosclerosis, Clinical Characteristics, and Treatment Patterns in Heart Failure: A Case-Control Study of Middle-Aged Adult Heart Failure Patients in Rural Kenya.Glob Heart. 2016 Mar;11(1):97-107. doi: 10.1016/j.gheart.2015.12.014. Glob Heart. 2016. PMID: 27102027 Free PMC article.
-
A review of clinical pharmacogenetics Studies in African populations.Per Med. 2020 Mar;17(2):155-170. doi: 10.2217/pme-2019-0110. Epub 2020 Mar 3. Per Med. 2020. PMID: 32125935 Free PMC article. Review.
References
-
- Lozano R, Naghavi M, Foreman K, Lim S, Shibuya K, Aboyans V, Abraham J, Adair T, Aggarwal R, Ahn SY, Alvarado M, Anderson HR, Anderson LM, Andrews KG, Atkinson C, Baddour LM, Barker‐Collo S, Bartels DH, Bell ML, Benjamin EJ, Bennett D, Bhalla K, Bikbov B, Bin Abdulhak A, Birbeck G, Blyth F, Bolliger I, Boufous S, Bucello C, Burch M, Burney P, Carapetis J, Chen H, Chou D, Chugh SS, Coffeng LE, Colan SD, Colquhoun S, Colson KE, Condon J, Connor MD, Cooper LT, Corriere M, Cortinovis M, de Vaccaro KC, Couser W, Cowie BC, Criqui MH, Cross M, Dabhadkar KC, Dahodwala N, De Leo D, Degenhardt L, Delossantos A, Denenberg J, Des Jarlais DC, Dharmaratne SD, Dorsey ER, Driscoll T, Duber H, Ebel B, Erwin PJ, Espindola P, Ezzati M, Feigin V, Flaxman AD, Forouzanfar MH, Fowkes FG, Franklin R, Fransen M, Freeman MK, Gabriel SE, Gakidou E, Gaspari F, Gillum RF, Gonzalez‐Medina D, Halasa YA, Haring D, Harrison JE, Havmoeller R, Hay RJ, Hoen B, Hotez PJ, Hoy D, Jacobsen KH, James SL, Jasrasaria R, Jayaraman S, Johns N, Karthikeyan G, Kassebaum N, Keren A, Khoo JP, Knowlton LM, Kobusingye O, Koranteng A, Krishnamurthi R, Lipnick M, Lipshultz SE, Ohno SL, Mabweijano J, MacIntyre MF, Mallinger L, March L, Marks GB, Marks R, Matsumori A, Matzopoulos R, Mayosi BM, McAnulty JH, McDermott MM, McGrath J, Mensah GA, Merriman TR, Michaud C, Miller M, Miller TR, Mock C, Mocumbi AO, Mokdad AA, Moran A, Mulholland K, Nair MN, Naldi L, Narayan KM, Nasseri K, Norman P, O'Donnell M, Omer SB, Ortblad K, Osborne R, Ozgediz D, Pahari B, Pandian JD, Rivero AP, Padilla RP, Perez‐Ruiz F, Perico N, Phillips D, Pierce K, Pope CA, III, Porrini E, Pourmalek F, Raju M, Ranganathan D, Rehm JT, Rein DB, Remuzzi G, Rivara FP, Roberts T, De León FR, Rosenfeld LC, Rushton L, Sacco RL, Salomon JA, Sampson U, Sanman E, Schwebel DC, Segui‐Gomez M, Shepard DS, Singh D, Singleton J, Sliwa K, Smith E, Steer A, Taylor JA, Thomas B, Tleyjeh IM, Towbin JA, Truelsen T, Undurraga EA, Venketasubramanian N, Vijayakumar L, Vos T, Wagner GR, Wang M, Wang W, Watt K, Weinstock MA, Weintraub R, Wilkinson JD, Woolf AD, Wulf S, Yeh PH, Yip P, Zabetian A, Zheng ZJ, Lopez AD, Murray CJ, AlMazroa MA, Memish ZA. Global and regional mortality from 235 causes of death for 20 age groups in 1990 and 2010: a systematic analysis for the Global Burden of Disease Study 2010. Lancet. 2012; 380:2095-2128. - PMC - PubMed
-
- Mensah GA. Ischaemic heart disease in Africa. Heart. 2008; 94:836-843. - PubMed
-
- Gaziano TA, Reddy KS, Paccaud F, Horton S, Chaturvedi V. In: Jamison DT, Breman J, Measham A, Alleyne G, Claeson M, Evans DB, Jha P, Mills A, Musgrove P. (eds.). Cardiovascular disease. Disease Control Priorities in Developing Countries. 20062nd edNew York, NY: Oxford University Press and World Bank; 2006. 645-662.
-
- Mayosi BM, Lawn JE, van Niekerk A, Bradshaw D, Abdool Karim SS, Coovadia HMLancet South Africa team. Health in South Africa: changes and challenges since 2009. Lancet. 2012; 380:2029-2043. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
