

Thin-section computed tomography detects long-term pulmonary sequelae 3 years after novel influenza A virus-associated pneumonia
- PMID: 25836610
- PMCID: PMC4834006
- DOI: 10.4103/0366-6999.154285
Thin-section computed tomography detects long-term pulmonary sequelae 3 years after novel influenza A virus-associated pneumonia
Abstract
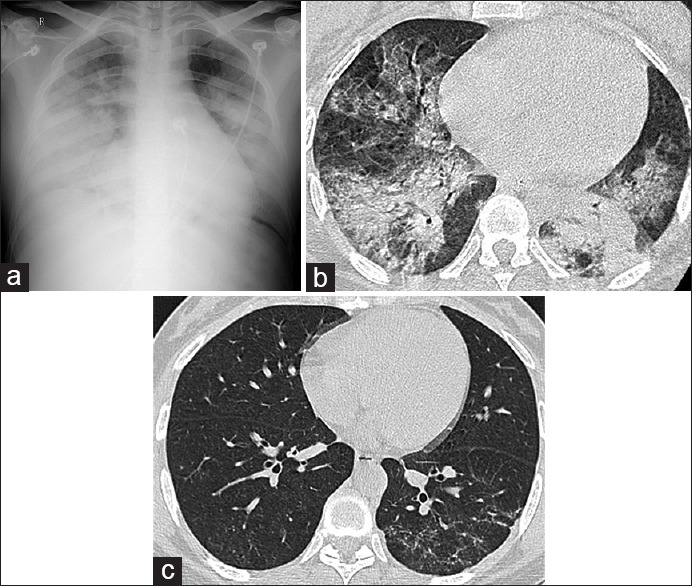
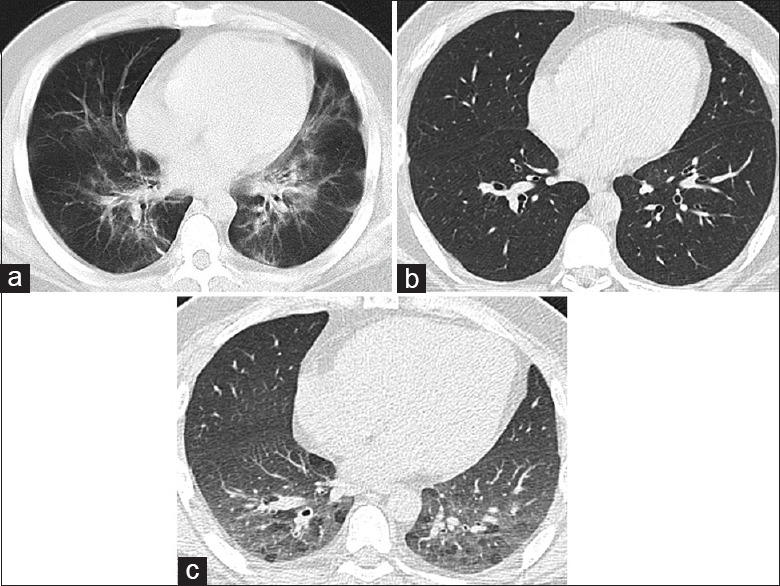
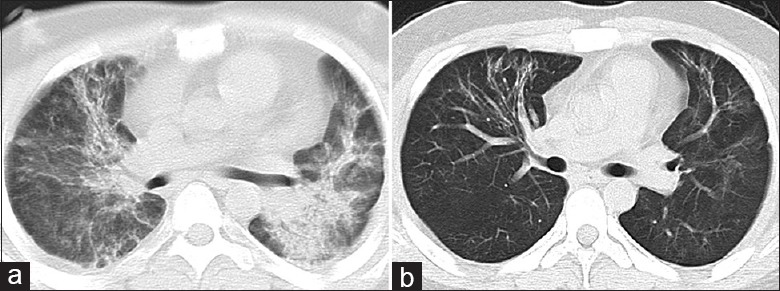
Background: The aim of this research was to evaluate long-term pulmonary sequelae on paired inspiration-expiration thin-section computed tomography (CT) scans 3 years after influenza A (H1N1) virus-associated pneumonia, and to analyze the affecting factors on pulmonary fibrosis.
Methods: Twenty-four patients hospitalized with H1N1 virus-associated pneumonia at our hospital between September 2009 and January 2010 were included. The patients underwent thin-section CT 3 years after recovery. Abnormal pulmonary lesion patterns (ground-glass opacity, consolidation, parenchymal bands, air trapping, and reticulation) and evidence of fibrosis (architectural distortion, traction bronchiectasis, or honeycombing) were evaluated on follow-up thin-section CT. Patients were assigned to Group 1 (with CT evidence of fibrosis) and Group 2 (without CT evidence of fibrosis). Demographics, rate of mechanical ventilation therapy, rate of intensive care unit admission, cumulative prednisolone-equivalent dose, laboratory tests results (maximum levels of alanine aminotransferase, aspartate transaminase [AST], lactate dehydrogenase [LDH], and creatine kinase [CK]), and peak radiographic opacification of 24 patients during the course of their illness in the hospital were compared between two groups.
Results: Parenchymal abnormality was present in 17 of 24 (70.8%) patients and fibrosis occurred in 10 of 24 (41.7%) patients. Patients in Group 1 (10/24; 41.7%) had a higher rate of mechanical ventilation therapy (Z = -2.340, P = 0.019), higher number of doses of cumulative prednisolone-equivalent (Z = -2.579, P = 0.010), higher maximum level of laboratory tests results (AST [Z = -2.140, P = 0.032], LDH [Z = -3.227, P = 0.001], and CK [Z = -3.345, P = 0.019]), and higher peak opacification on chest radiographs (Z = -2.743, P = 0.006) than patients in group 2 (14/24; 58.3%).
Conclusions: H1N1 virus-associated pneumonia frequently is followed by long-term pulmonary sequelae, including fibrotic changes, in lung parenchyma. Patients who need more steroid therapy, need more mechanical ventilation therapy, had higher laboratory tests results (maximum levels of AST, LDH, and CK), and had higher peak opacification on chest radiographs during treatment are more likely to develop lung fibrosis.
Conflict of interest statement
Figures
Similar articles
-
Thin-section CT in patients with severe acute respiratory syndrome following hospital discharge: preliminary experience.Radiology. 2003 Sep;228(3):810-5. doi: 10.1148/radiol.2283030726. Epub 2003 Jun 12. Radiology. 2003. PMID: 12805557
-
Chest Radiological Findings of Patients With Severe H1N1 Pneumonia Requiring Intensive Care.J Intensive Care Med. 2016 Jan;31(1):51-60. doi: 10.1177/0885066614538753. Epub 2014 Jun 12. J Intensive Care Med. 2016. PMID: 24923491
-
[Report of 2 cases of novel influenza A (H1N1) virus infection complicated with pneumonia and hypoxemia].Zhonghua Jie He He Hu Xi Za Zhi. 2010 Feb;33(2):86-92. Zhonghua Jie He He Hu Xi Za Zhi. 2010. PMID: 20367946 Chinese.
-
Chest CT Lung Abnormalities 1 Year after COVID-19: A Systematic Review and Meta-Analysis.Radiology. 2023 Jul;308(1):e230535. doi: 10.1148/radiol.230535. Radiology. 2023. PMID: 37404150
-
Approach to ground-glass opacification of the lung.Semin Ultrasound CT MR. 2002 Aug;23(4):302-23. doi: 10.1016/s0887-2171(02)90019-3. Semin Ultrasound CT MR. 2002. PMID: 12465687 Review.
Cited by
-
Possible Role of Matrix Metalloproteinases and TGF-β in COVID-19 Severity and Sequelae.J Interferon Cytokine Res. 2022 Aug;42(8):352-368. doi: 10.1089/jir.2021.0222. Epub 2022 May 31. J Interferon Cytokine Res. 2022. PMID: 35647937 Free PMC article. Review.
-
Assessment of 1-year Outcomes in Survivors of Severe Acute Respiratory Distress Syndrome Receiving Extracorporeal Membrane Oxygenation or Mechanical Ventilation: A Prospective Observational Study.Chin Med J (Engl). 2017 May 20;130(10):1161-1168. doi: 10.4103/0366-6999.205847. Chin Med J (Engl). 2017. PMID: 28485315 Free PMC article.
-
Quantitative inspiratory-expiratory chest CT findings in COVID-19 survivors at the 6-month follow-up.Sci Rep. 2022 May 5;12(1):7402. doi: 10.1038/s41598-022-11237-1. Sci Rep. 2022. PMID: 35513692 Free PMC article.
-
Low-dose cadmium potentiates lung inflammatory response to 2009 pandemic H1N1 influenza virus in mice.Environ Int. 2019 Jun;127:720-729. doi: 10.1016/j.envint.2019.03.054. Epub 2019 Apr 15. Environ Int. 2019. PMID: 30999129 Free PMC article.
-
COVID-19 and pulmonary fibrosis: A potential role for lung epithelial cells and fibroblasts.Immunol Rev. 2021 Jul;302(1):228-240. doi: 10.1111/imr.12977. Epub 2021 May 24. Immunol Rev. 2021. PMID: 34028807 Free PMC article. Review.
References
-
- Perez-Padilla R, de la Rosa-Zamboni D, Ponce de Leon S, Hernandez M, Quiñones-Falconi F, Bautista E, et al. Pneumonia and respiratory failure from swine-origin influenza A (H1N1) in Mexico. N Engl J Med. 2009;361:680–9. - PubMed
-
- Roch A, Lepaul-Ercole R, Grisoli D, Bessereau J, Brissy O, Castanier M, et al. Extracorporeal membrane oxygenation for severe influenza A (H1N1) acute respiratory distress syndrome: A prospective observational comparative study. Intensive Care Med. 2010;36:1899–905. - PubMed
-
- Agarwal PP, Cinti S, Kazerooni EA. Chest radiographic and CT findings in novel swine-origin influenza A (H1N1) virus (S-OIV) infection. AJR Am J Roentgenol. 2009;193:1488–93. - PubMed
-
- Chu WC, Li AM, Ng AW, So HK, Lam WW, Lo KL, et al. Thin-section CT 12 months after the diagnosis of severe acute respiratory syndrome in pediatric patients. AJR Am J Roentgenol. 2006;186:1707–14. - PubMed
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
