

J wave syndromes: a decade of progress
- PMID: 25836620
- PMCID: PMC4834016
- DOI: 10.4103/0366-6999.154320
J wave syndromes: a decade of progress
Abstract
Objective: The objective was to provide a brief history of J wave syndromes and to summarize our current understanding of their molecular, ionic, cellular mechanisms, and clinical features. We will also discuss the existing debates and further direction in basic and clinical research for J wave syndromes.
Data sources: The publications on key words of "J wave syndromes", "early repolarization syndrome (ERS)", "Brugada syndrome (BrS)" and "ST-segment elevation myocardial infarction (STEMI)" were comprehensively reviewed through search of the PubMed literatures without restriction on the publication date.
Study selection: Original articles, reviews and other literatures concerning J wave syndromes, ERS, BrS and STEMI were selected.
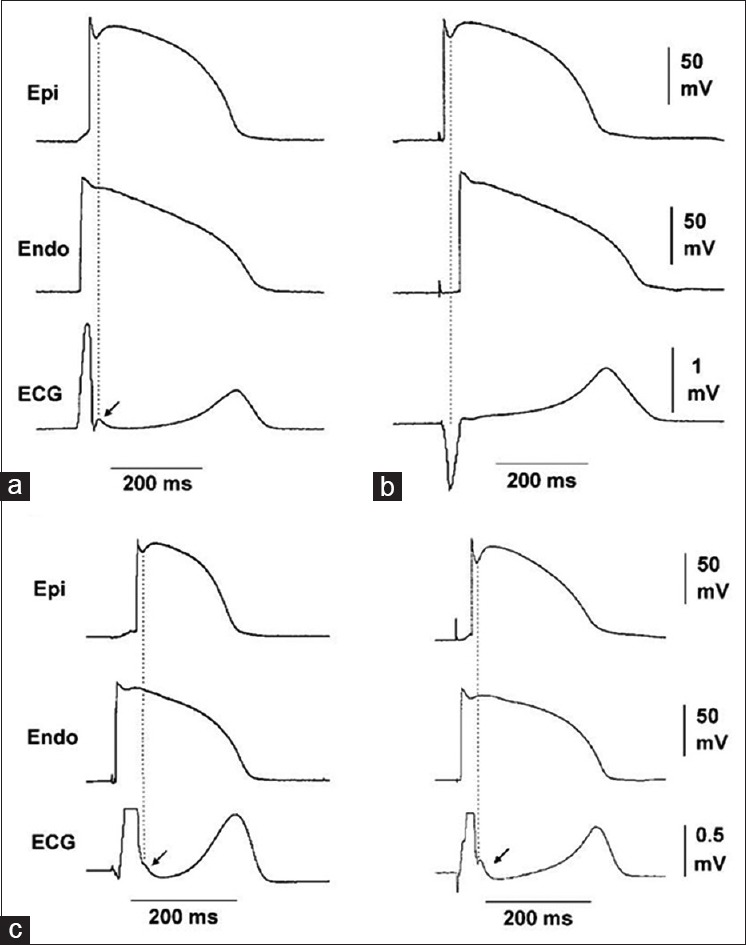
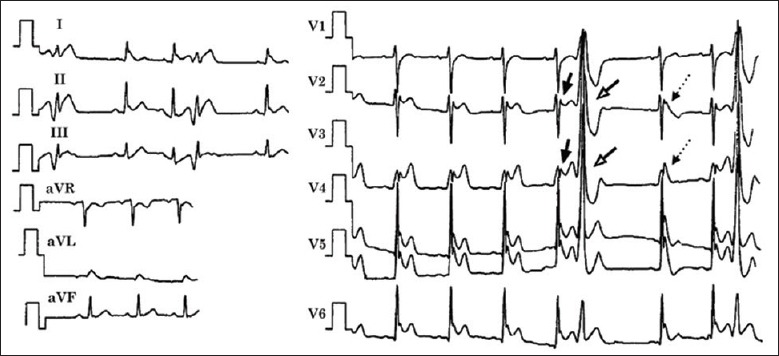
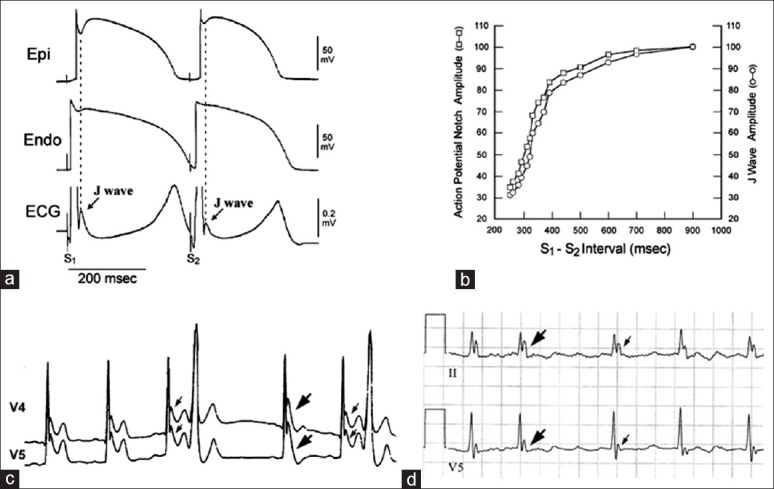
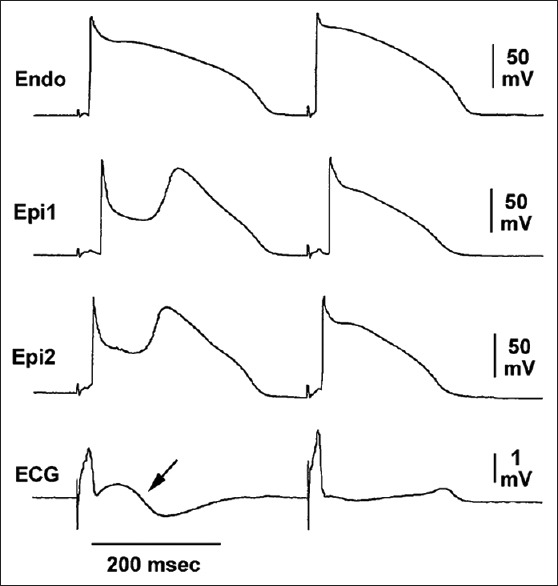
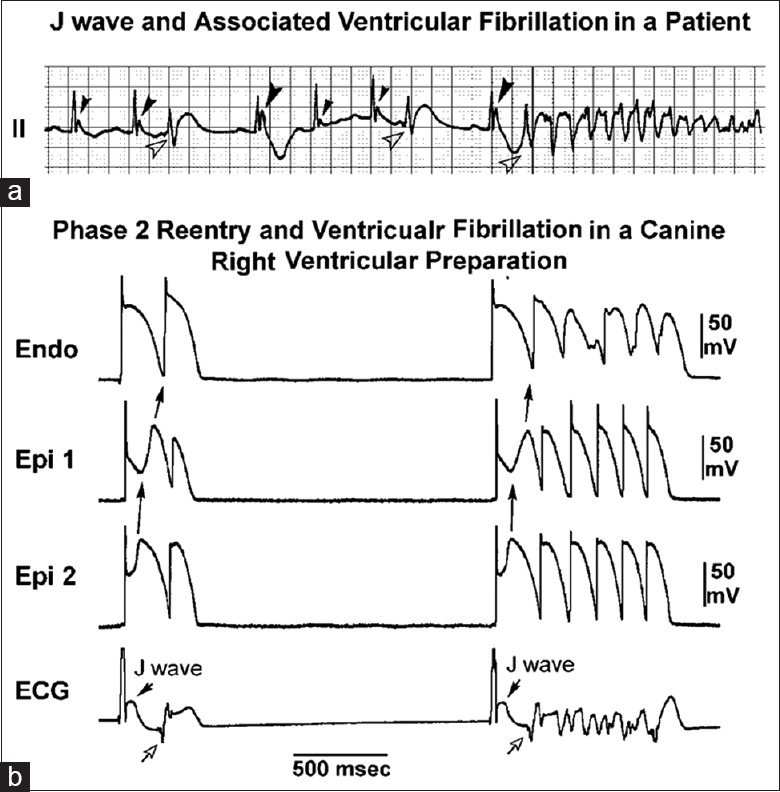
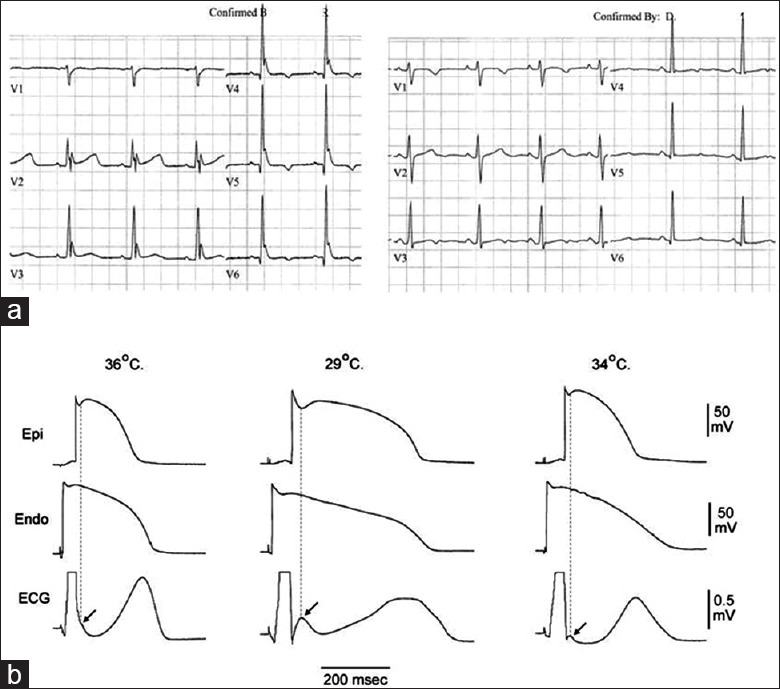
Results: J wave syndromes were firstly defined by Yan et al. in a Chinese journal a decade ago, which represent a spectrum of variable phenotypes characterized by appearance of prominent electrocardiographic J wave including ERS, BrS and ventricular fibrillation (VF) associated with hypothermia and acute STEMI. J wave syndromes can be inherited or acquired and are mechanistically linked to amplification of the transient outward current (I to )-mediated J waves that can lead to phase 2 reentry capable of initiating VF.
Conclusions: J wave syndromes are a group of newly highlighted clinical entities that share similar molecular, ionic and cellular mechanism and marked by amplified J wave on the electrocardiogram and a risk of VF. The clinical challenge ahead is to identify the patients with J wave syndromes who are at risk for sudden cardiac death and determine the alternative therapeutic strategies to reduce mortality.
Conflict of interest statement
Figures
Similar articles
-
J wave syndromes: molecular and cellular mechanisms.J Electrocardiol. 2013 Nov-Dec;46(6):510-8. doi: 10.1016/j.jelectrocard.2013.08.006. Epub 2013 Sep 6. J Electrocardiol. 2013. PMID: 24011992 Free PMC article. Review.
-
J wave syndromes as a cause of malignant cardiac arrhythmias.Pacing Clin Electrophysiol. 2018 Jul;41(7):684-699. doi: 10.1111/pace.13408. Epub 2018 Jun 30. Pacing Clin Electrophysiol. 2018. PMID: 29870068 Free PMC article. Review.
-
Idiopathic ventricular fibrillation, early repolarization and other J wave-related ventricular fibrillation syndromes: from an electrocardiographic enigma to an electrophysiologic dogma.Circ J. 2012;76(12):2723-31. doi: 10.1253/circj.cj-12-1306. Epub 2012 Nov 7. Circ J. 2012. PMID: 23131759 Review.
-
Acacetin suppresses the electrocardiographic and arrhythmic manifestations of the J wave syndromes.PLoS One. 2020 Nov 24;15(11):e0242747. doi: 10.1371/journal.pone.0242747. eCollection 2020. PLoS One. 2020. PMID: 33232375 Free PMC article.
-
Early repolarisation and J wave syndromes.Indian Heart J. 2014 Jul-Aug;66(4):443-52. doi: 10.1016/j.ihj.2014.06.002. Epub 2014 Aug 5. Indian Heart J. 2014. PMID: 25173204 Free PMC article. Review.
Cited by
-
Broad Electrocardiogram Syndromes Spectrum: From Common Emergencies to Particular Electrical Heart Disorders.J Pers Med. 2022 Oct 22;12(11):1754. doi: 10.3390/jpm12111754. J Pers Med. 2022. PMID: 36573711 Free PMC article. Review.
-
Relationship Between an Ischaemic J Wave Pattern and Ventricular Fibrillation in ST-Elevation Myocardial Infarction Patients.Int J Gen Med. 2021 Nov 23;14:8725-8735. doi: 10.2147/IJGM.S337638. eCollection 2021. Int J Gen Med. 2021. PMID: 34849013 Free PMC article.
-
Predictive effect of J waves on cardiac compression and clinical prognosis of esophageal tumors: a retrospective study.J Gastrointest Oncol. 2022 Jun;13(3):923-934. doi: 10.21037/jgo-22-371. J Gastrointest Oncol. 2022. PMID: 35837153 Free PMC article.
-
J Wave Syndromes: History and Current Controversies.Korean Circ J. 2016 Sep;46(5):601-609. doi: 10.4070/kcj.2016.46.5.601. Epub 2016 Sep 28. Korean Circ J. 2016. PMID: 27721848 Free PMC article. Review.
-
Heart rate variability in children and adolescents with incidentally found early repolarization pattern.BMC Cardiovasc Disord. 2025 May 8;25(1):356. doi: 10.1186/s12872-025-04824-3. BMC Cardiovasc Disord. 2025. PMID: 40340710 Free PMC article.
References
-
- Yan GX, Yao QH, Wang DQ, Cui CC. J wave and J wave syndromes (in Chinese) Chin J Card Arrhythm. 2004;8:360–5.
-
- Shu J, Zhu T, Yang L, Cui C, Yan GX. ST-segment elevation in the early repolarization syndrome, idiopathic ventricular fibrillation, and the Brugada syndrome: Cellular and clinical linkage. J Electrocardiol. 2005;38(4 Suppl):26–32. - PubMed
-
- Badri M, Patel A, Yan G. Cellular and ionic basis of J-wave syndromes. Trends Cardiovasc Med. 2015;25:12–21. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
