

Size distribution of air bubbles entering the brain during cardiac surgery
- PMID: 25837519
- PMCID: PMC4383554
- DOI: 10.1371/journal.pone.0122166
Size distribution of air bubbles entering the brain during cardiac surgery
Abstract
Background: Thousands of air bubbles enter the cerebral circulation during cardiac surgery, but whether high numbers of bubbles explain post-operative cognitive decline is currently controversial. This study estimates the size distribution of air bubbles and volume of air entering the cerebral arteries intra-operatively based on analysis of transcranial Doppler ultrasound data.
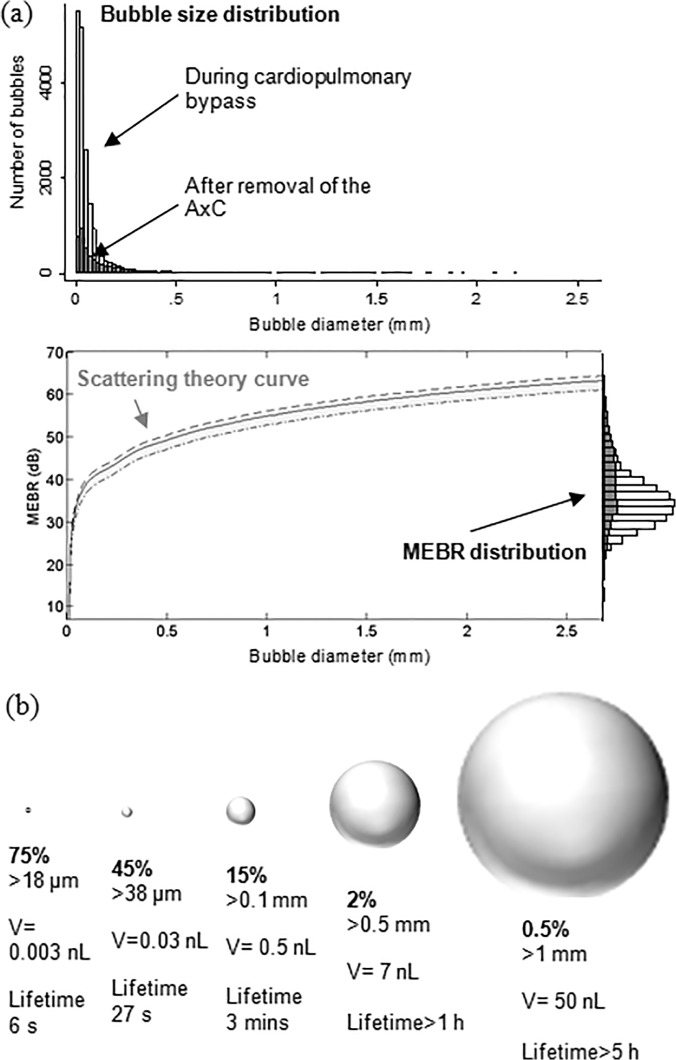
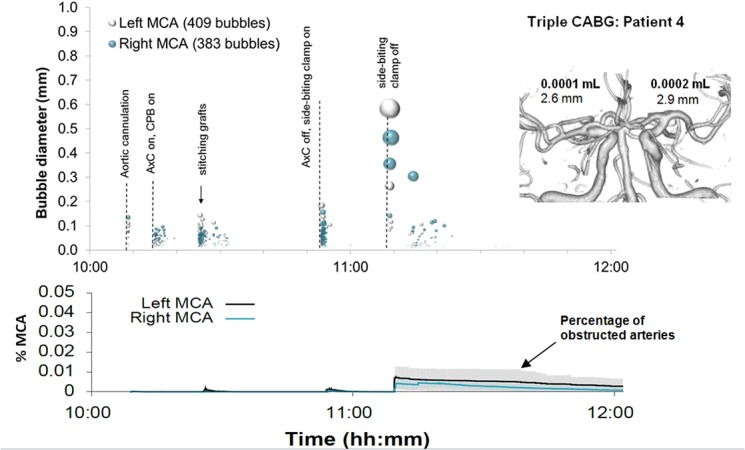
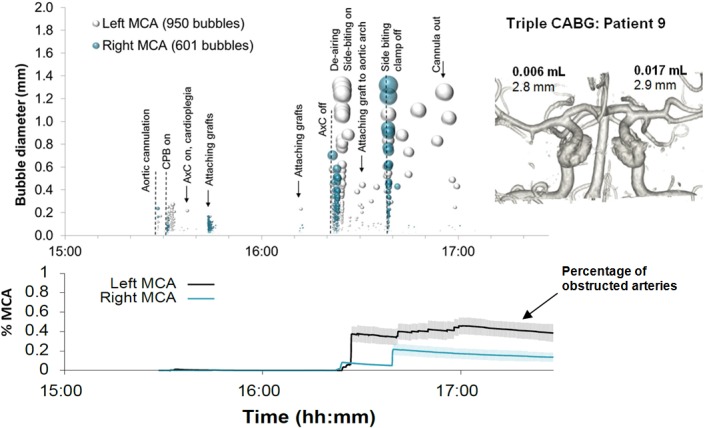
Methods: Transcranial Doppler ultrasound recordings from ten patients undergoing heart surgery were analysed for the presence of embolic signals. The backscattered intensity of each embolic signal was modelled based on ultrasound scattering theory to provide an estimate of bubble diameter. The impact of showers of bubbles on cerebral blood-flow was then investigated using patient-specific Monte-Carlo simulations to model the accumulation and clearance of bubbles within a model vasculature.
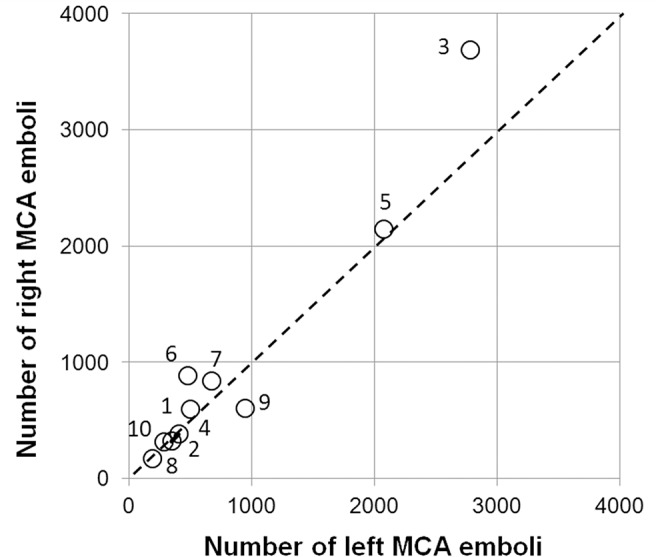
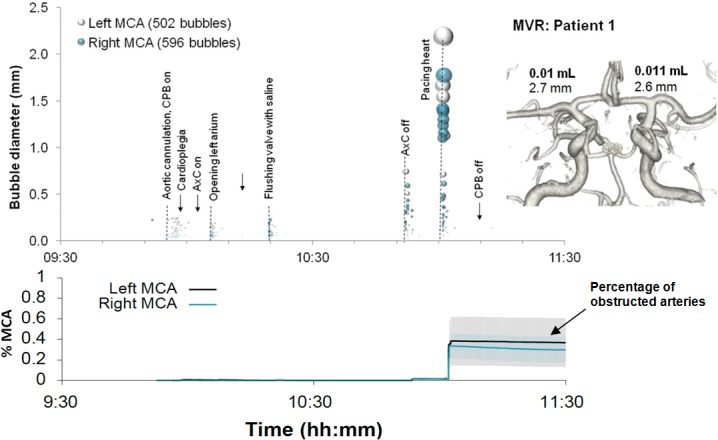
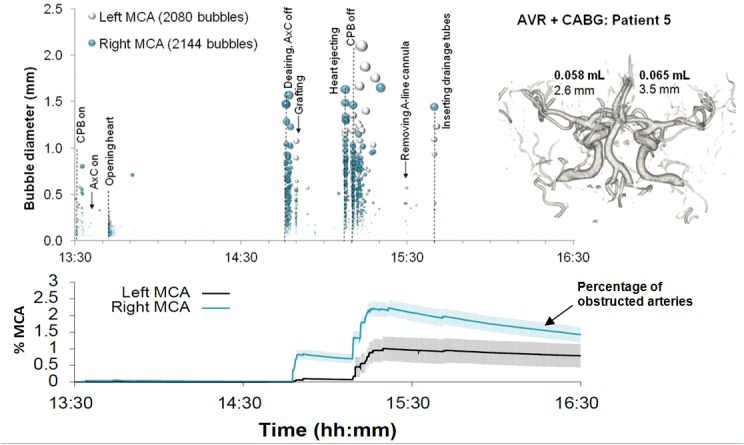
Results: Analysis of Doppler ultrasound recordings revealed a minimum of 371 and maximum of 6476 bubbles entering the middle cerebral artery territories during surgery. This was estimated to correspond to a total volume of air ranging between 0.003 and 0.12 mL. Based on analysis of a total of 18667 embolic signals, the median diameter of bubbles entering the cerebral arteries was 33 μm (IQR: 18 to 69 μm). Although bubble diameters ranged from ~5 μm to 3.5 mm, the majority (85%) were less than 100 μm. Numerous small bubbles detected during cardiopulmonary bypass were estimated by Monte-Carlo simulation to be benign. However, during weaning from bypass, showers containing large macro-bubbles were observed, which were estimated to transiently affect up to 2.2% of arterioles.
Conclusions: Detailed analysis of Doppler ultrasound data can be used to provide an estimate of bubble diameter, total volume of air, and the likely impact of embolic showers on cerebral blood flow. Although bubbles are alarmingly numerous during surgery, our simulations suggest that the majority of bubbles are too small to be harmful.
Conflict of interest statement
Figures
References
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
