

Lyme carditis--diagnosis, treatment and prognosis
- PMID: 25838022
- PMCID: PMC4395762
- DOI: 10.3238/arztebl.2015.0202
Lyme carditis--diagnosis, treatment and prognosis
Abstract
Background: There are 60,000 to 100,000 new cases of borreliosis in Germany each year. This infectious disease most commonly affects the skin, joints, and nervous system. Lyme carditis is a rare manifestation with potentially lethal complications.
Methods: This review is based on selected publications on the clinical manifestations, diagnosis, and treatment of Lyme carditis, and on the authors' scientific and clinical experience.
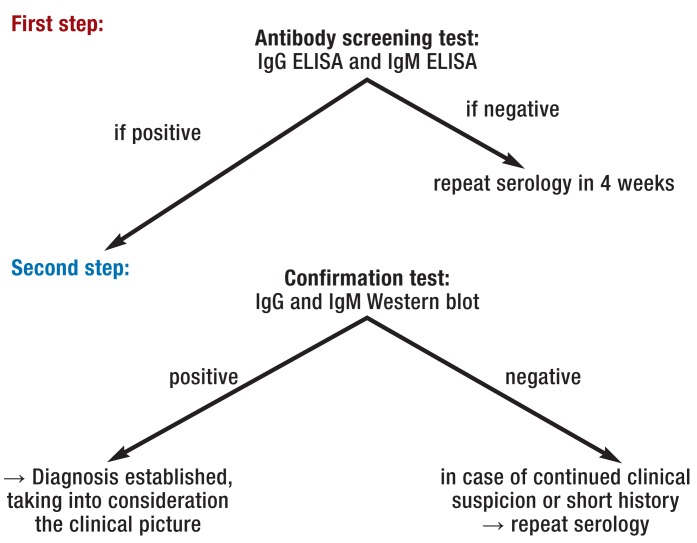
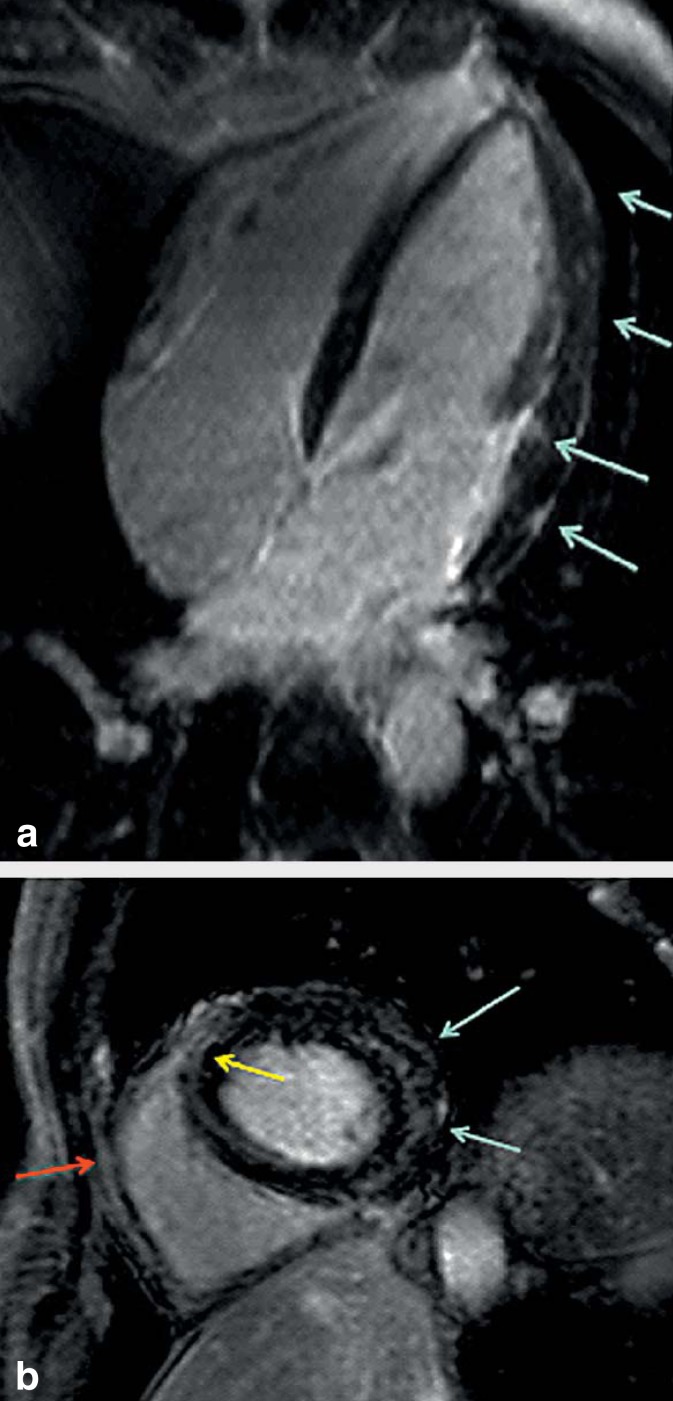
Results: Lyme carditis is seen in 4% to 10% of all patients with Lyme borreliosis. Whenever the clinical suspicion of Lyme carditis arises, an ECG is mandatory for the detection or exclusion of an atrioventricular conduction block. Patients with a PQ interval longer than 300 ms need continuous ECG monitoring. 90% of patients with Lyme carditis develop cardiac conduction abnormalities, and 60% develop signs of perimyocarditis. Borrelia serology (ELISA) may still be negative in the early phase of the condition, but is always positive in later phases. Cardiac MRI can be used to confirm the diagnosis and to monitor the patient's subsequent course. The treatment of choice is with antibiotics, preferably ceftriaxone. The cardiac conduction disturbances are usually reversible, and the implantation of a permanent pacemaker is only exceptionally necessary. There is no clear evidence at present for an association between borreliosis and the later development of a dilated cardiomyopathy. When Lyme carditis is treated according to the current guidelines, its prognosis is highly favorable.
Conclusion: Lyme carditis is among the rarer manifestations of Lyme borreliosis but must nevertheless be considered prominently in differential diagnosis because of the potentially severe cardiac arrhythmias that it can cause.
Figures

References
-
- Stanek G, Wormser GP, Gray J, Strle F. Lyme borreliosis. Lancet. 2012;379:461–473. - PubMed
-
- Dubrey SW, Bhatia A, Woodham S, Rakowicz W. Lyme disease in the United Kingdom. Postgrad Med J. 2014;90:33–42. - PubMed
-
- Frank C, Faber M, Hellenbrand W, Wilking H, Stark K. Wichtige, durch Vektoren übertragene Infektionskrankheiten beim Menschen in Deutschland. Epidemiologische Aspekte. Bundesgesundheitsbl. 2014;5:1–10. - PubMed
-
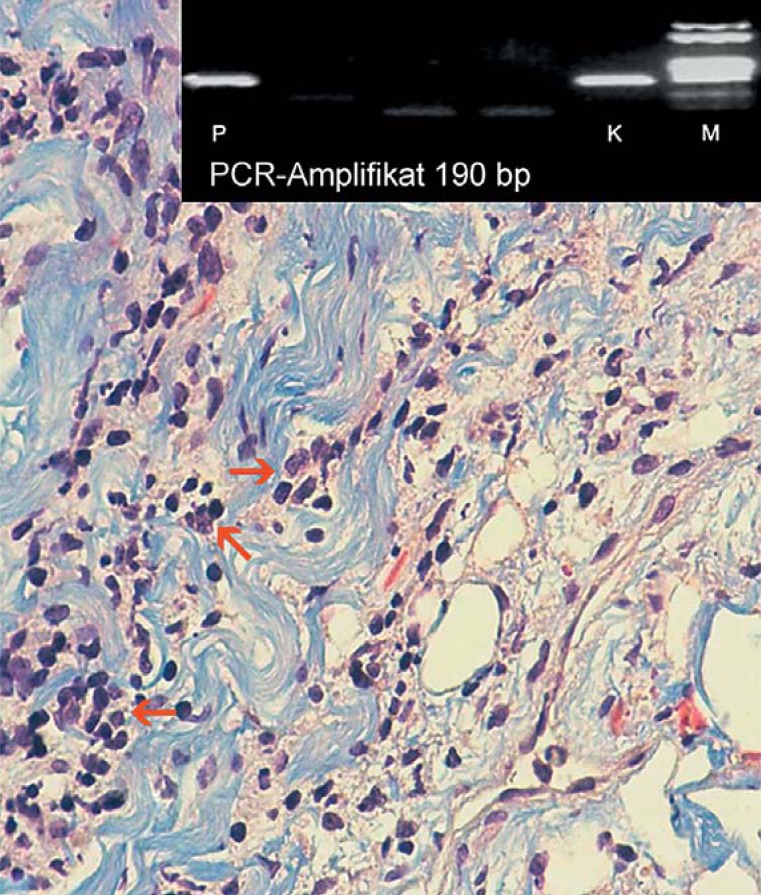
- Marcus LC, Steere AC, Duray PH, Anderson AE, Mahoney EB. Fatal pancarditis in a patient with coexistent lyme disease and babesiosis. Demonstration of spirochetes in the myocardium. Ann Intern Med. 1985;103:374–376. - PubMed
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical