

Immunopathology of chronic rhinosinusitis
- PMID: 25838086
- PMCID: PMC4675657
- DOI: 10.1016/j.alit.2014.12.006
Immunopathology of chronic rhinosinusitis
Abstract
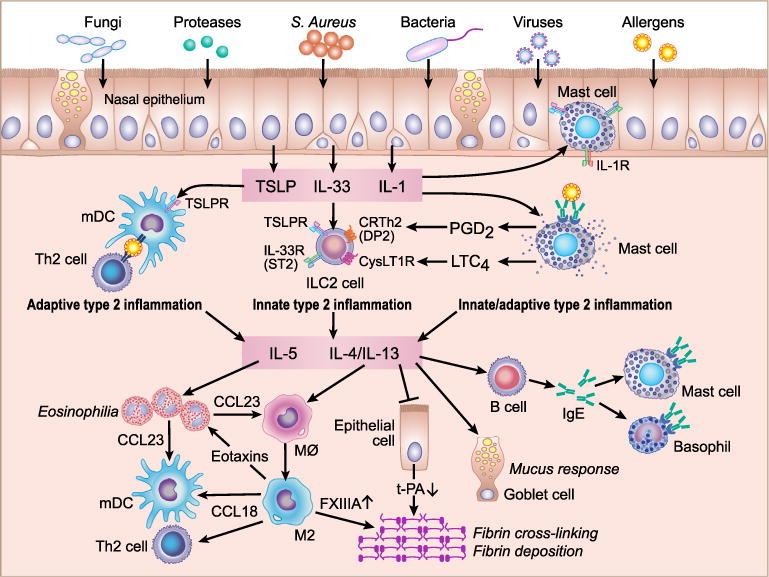
Chronic rhinosinusitis (CRS) is a heterogeneous disease characterized by local inflammation of the upper airways and sinuses which persists for at least 12 weeks. CRS can be divided into two phenotypes dependent on the presence of nasal polyps (NPs); CRS with NPs (CRSwNP) and CRS without NPs (CRSsNP). Immunological patterns in the two diseases are known to be different. Inflammation in CRSsNP is rarely investigated and limited studies show that CRSsNP is characterized by type 1 inflammation. Inflammation in CRSwNP is well investigated and CRSwNP in Western countries shows type 2 inflammation and eosinophilia in NPs. In contrast, mixed inflammatory patterns are found in CRSwNP in Asia and the ratio of eosinophilic NPs and non-eosinophilic NPs is almost 50:50 in these countries. Inflammation in eosinophilic NPs is mainly controlled by type 2 cytokines, IL-5 and IL-13, which can be produced from several immune cells including Th2 cells, mast cells and group 2 innate lymphoid cells (ILC2s) that are all elevated in eosinophilic NPs. IL-5 strongly induces eosinophilia. IL-13 activates macrophages, B cells and epithelial cells to induce recruitment of eosinophils and Th2 cells, IgE mediated reactions and remodeling. Epithelial derived cytokines, TSLP, IL-33 and IL-1 can directly and indirectly control type 2 cytokine production from these cells in eosinophilic NPs. Recent clinical trials showed the beneficial effect on eosinophilic NPs and/or asthma by monoclonal antibodies against IL-5, IL-4Rα, IgE and TSLP suggesting that they can be therapeutic targets for eosinophilic CRSwNP.
Keywords: Chronic rhinosinusitis; Eosinophilia; Nasal polyps; TSLP; Type 2 inflammation.
Copyright © 2015 Japanese Society of Allergology. Production and hosting by Elsevier B.V. All rights reserved.
Conflict of interest statement
Conflict of interest
The author has no conflict of interest to declare.
Figures
References
-
- Bhattacharyya N. Incremental health care utilization and expenditures for chronic rhinosinusitis in the United States. Ann Otol Rhinol Laryngol. 2011;120:423–7. - PubMed
-
- Fokkens WJ, Lund VJ, Mullol J, Bachert C, Alobid I, Baroody F, et al. European position paper on rhinosinusitis and nasal polyps 2012. Rhinol Suppl. 2012:1–298. 3 p preceding table of contents. - PubMed
-
- Bachert C, Van Bruaene N, Toskala E, Zhang N, Olze H, Scadding G, et al. Important research questions in allergy and related diseases: 3-chronic rhinosinusitis and nasal polyposis e a GALEN study. Allergy. 2009;64:520–33. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
