

Differences Between Colon Cancer Primaries and Metastases Using a Molecular Assay for Tumor Radiation Sensitivity Suggest Implications for Potential Oligometastatic SBRT Patient Selection
- PMID: 25838188
- PMCID: PMC4481172
- DOI: 10.1016/j.ijrobp.2015.01.036
Differences Between Colon Cancer Primaries and Metastases Using a Molecular Assay for Tumor Radiation Sensitivity Suggest Implications for Potential Oligometastatic SBRT Patient Selection
Abstract
Purpose: We previously developed a multigene expression model of tumor radiation sensitivity index (RSI) with clinical validation in multiple independent cohorts (breast, rectal, esophageal, and head and neck patients). The purpose of this study was to assess differences between RSI scores in primary colon cancer and metastases.
Methods and materials: Patients were identified from our institutional review board-approved prospective observational protocol. A total of 704 metastatic and 1362 primary lesions were obtained from a de-identified metadata pool. RSI was calculated using the previously published rank-based algorithm. An independent cohort of 29 lung or liver colon metastases treated with 60 Gy in 5 fractions stereotactic body radiation therapy (SBRT) was used for validation.
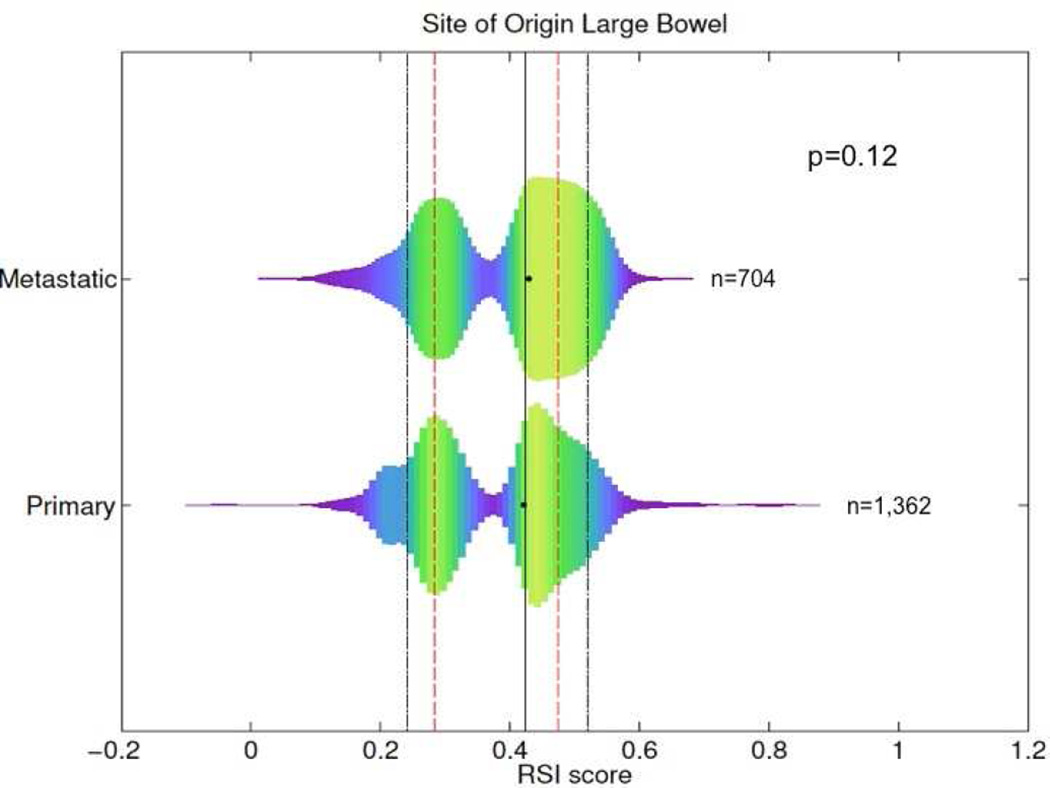
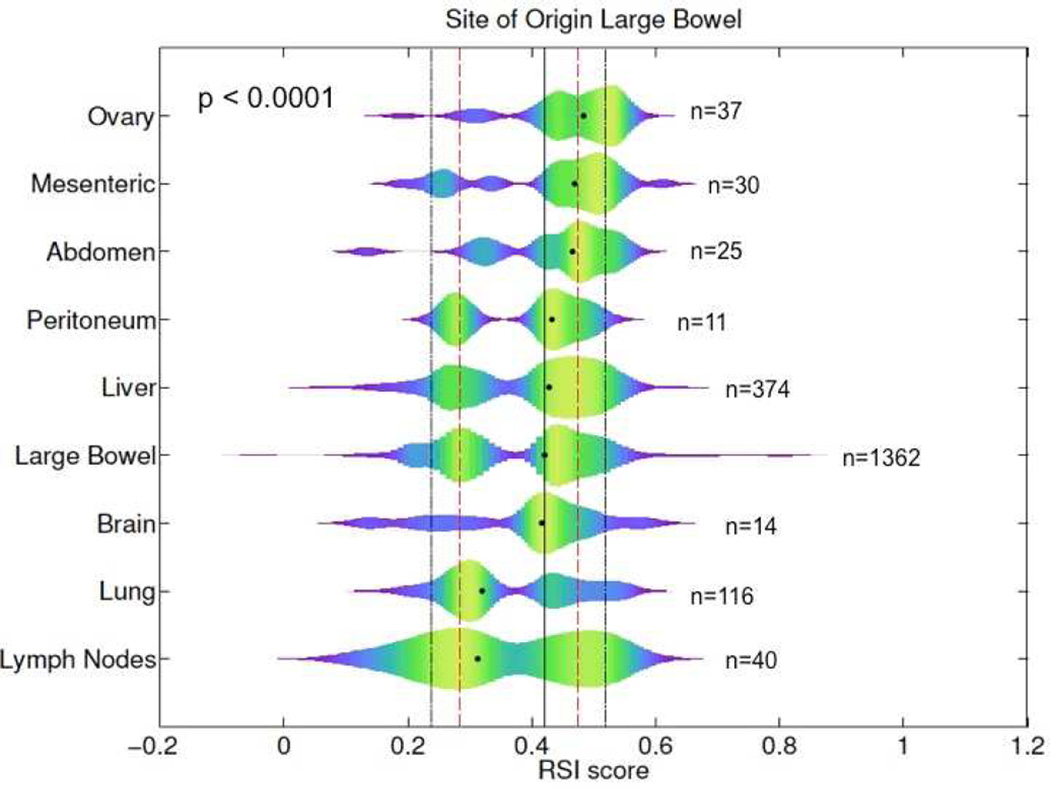
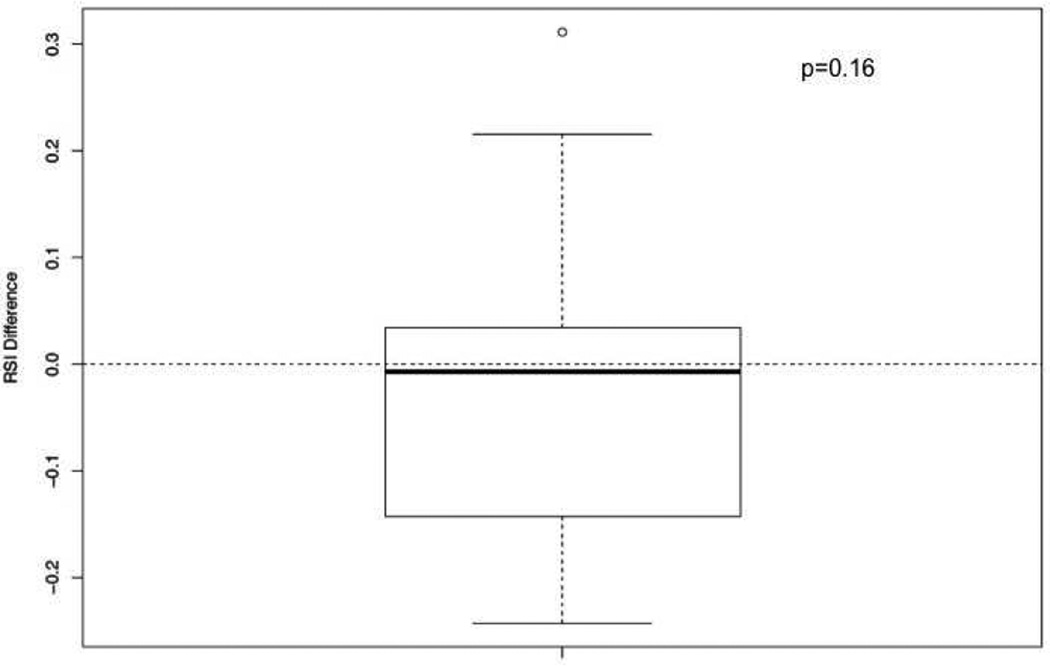
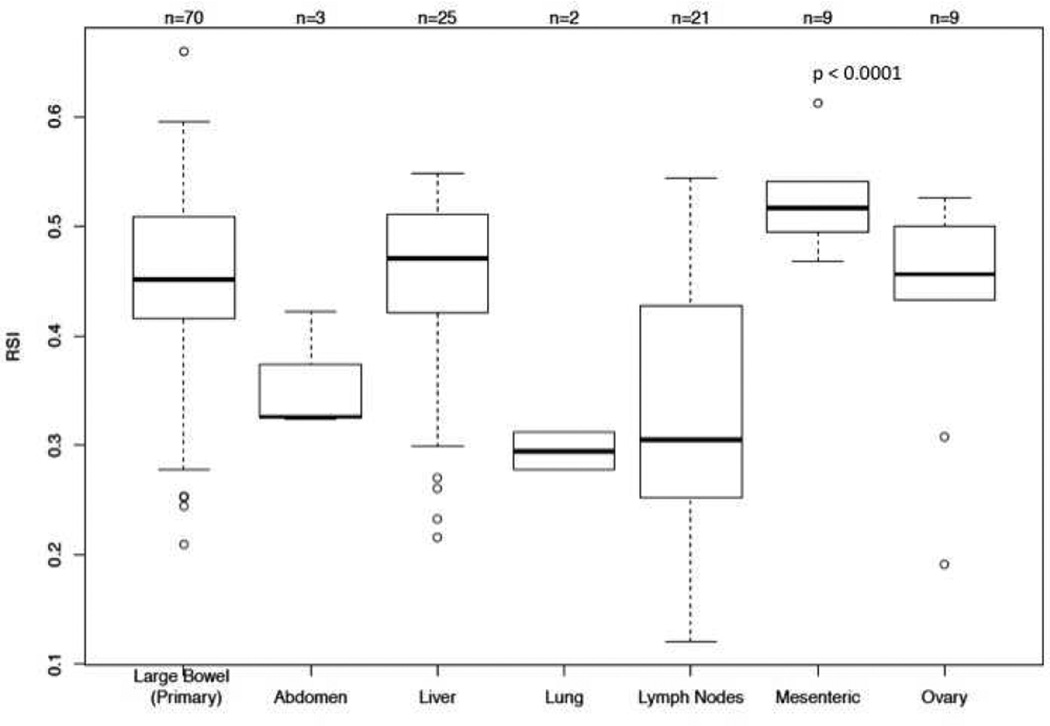
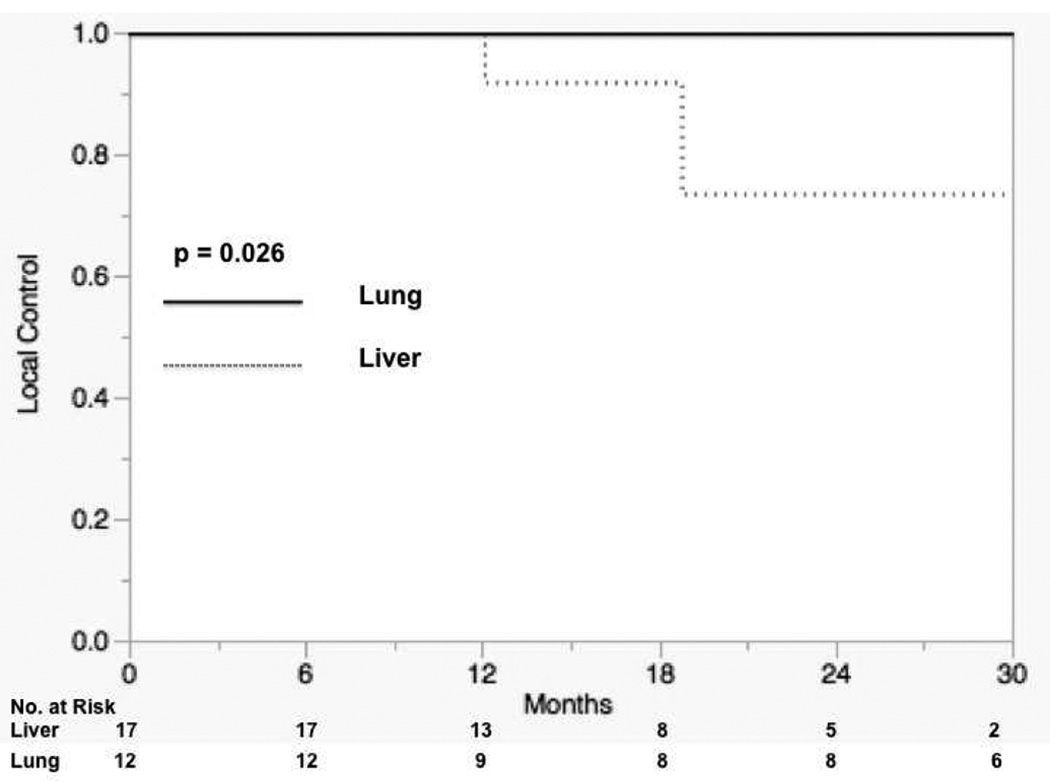
Results: The most common sites of metastases included liver (n=374; 53%), lung (n=116; 17%), and lymph nodes (n=40; 6%). Sixty percent of metastatic tumors, compared with 54% of primaries, were in the RSI radiation-resistant peak, suggesting metastatic tumors may be slightly more radiation resistant than primaries (P=.01). In contrast, when we analyzed metastases based on anatomical site, we uncovered large differences in RSI. The median RSIs for metastases in descending order of radiation resistance were ovary (0.48), abdomen (0.47), liver (0.43), brain (0.42), lung (0.32), and lymph nodes (0.31) (P<.0001). These findings were confirmed when the analysis was restricted to lesions from the same patient (n=139). In our independent cohort of treated lung and liver metastases, lung metastases had an improved local control rate compared to that in patients with liver metastases (2-year local control rate of 100% vs 73.0%, respectively; P=.026).
Conclusions: Assessment of radiation sensitivity between primary and metastatic tissues of colon cancer histology revealed significant differences based on anatomical location of metastases. These initial results warrant validation in a larger clinical cohort.
Copyright © 2015 Elsevier Inc. All rights reserved.
Conflict of interest statement
Figures
Comment in
-
Personalized Medicine in Radiation Oncology--A Work in Progress.Int J Radiat Oncol Biol Phys. 2015 Jul 15;92(4):843-5. doi: 10.1016/j.ijrobp.2015.04.020. Int J Radiat Oncol Biol Phys. 2015. PMID: 26104937 No abstract available.
References
-
- Fong Y, Cohen AM, Fortner JG, Enker WE, Turnbull AD, Coit DG, Marrero AM, Prasad M, Blumgart LH, Brennan MF. Liver resection for colorectal metastases. Journal of clinical oncology : official journal of the American Society of Clinical Oncology. 1997;15:938–946. - PubMed
-
- Long-term results of lung metastasectomy: Prognostic analyses based on 5206 cases. The international registry of lung metastases. The Journal of thoracic and cardiovascular surgery. 1997;113:37–49. - PubMed
-
- Aloia TA, Vauthey JN, Loyer EM, Ribero D, Pawlik TM, Wei SH, Curley SA, Zorzi D, Abdalla EK. Solitary colorectal liver metastasis: Resection determines outcome. Archives of surgery. 2006;141:460–466. discussion 466-467. - PubMed
-
- Patchell RA, Tibbs PA, Regine WF, Dempsey RJ, Mohiuddin M, Kryscio RJ, Markesbery WR, Foon KA, Young B. Postoperative radiotherapy in the treatment of single metastases to the brain: A randomized trial. JAMA : the journal of the American Medical Association. 1998;280:1485–1489. - PubMed
-
- Andrews DW, Scott CB, Sperduto PW, Flanders AE, Gaspar LE, Schell MC, Werner-Wasik M, Demas W, Ryu J, Bahary JP, Souhami L, Rotman M, Mehta MP, Curran WJ., Jr Whole brain radiation therapy with or without stereotactic radiosurgery boost for patients with one to three brain metastases: Phase iii results of the rtog 9508 randomised trial. Lancet. 2004;363:1665–1672. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
