

Pediatric Small Bowel Crohn Disease: Correlation of US and MR Enterography
- PMID: 25839736
- PMCID: PMC4450979
- DOI: 10.1148/rg.2015140002
Pediatric Small Bowel Crohn Disease: Correlation of US and MR Enterography
Abstract
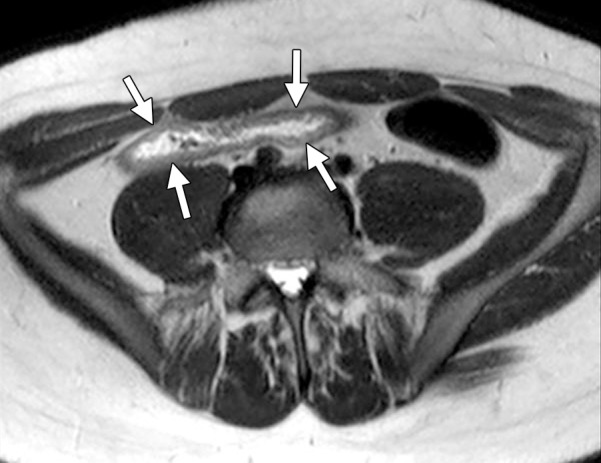
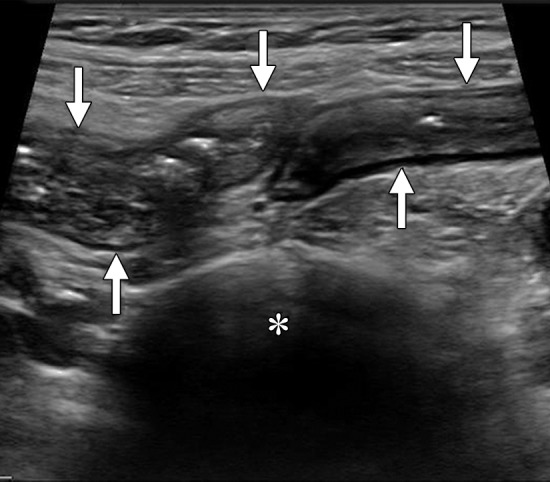
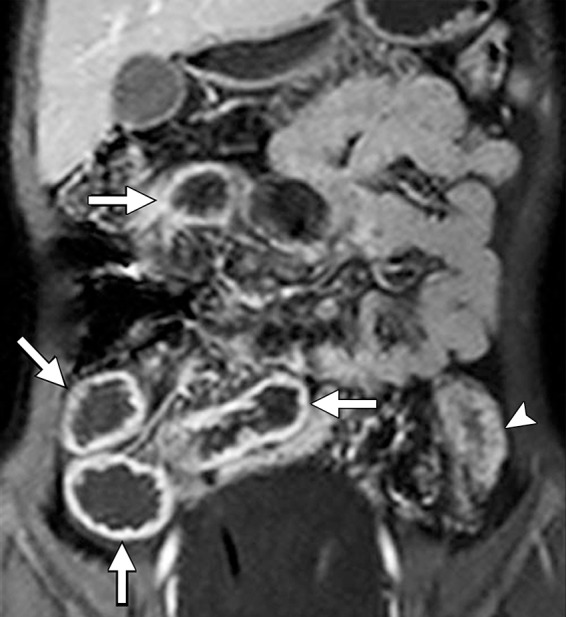
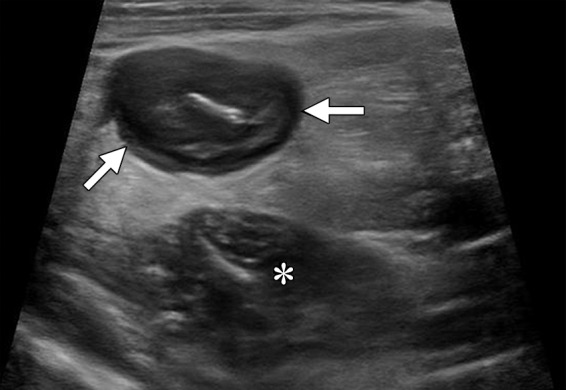
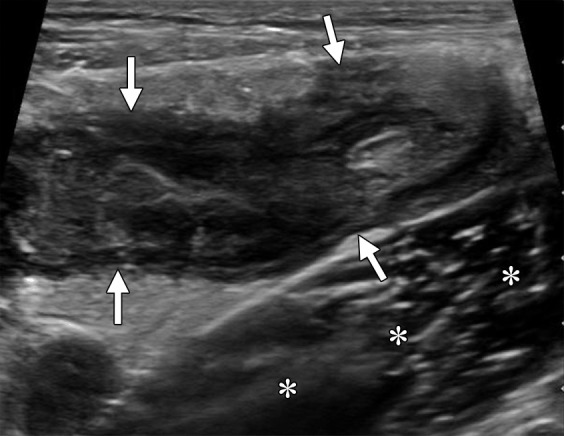
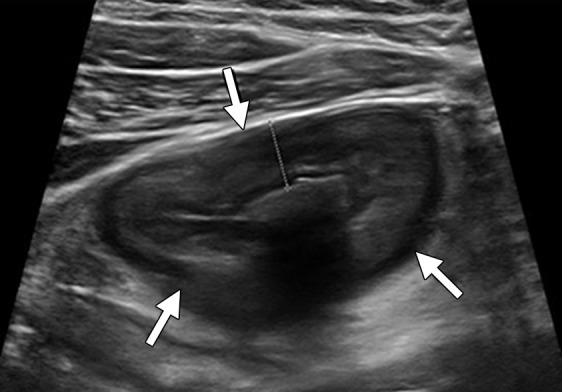
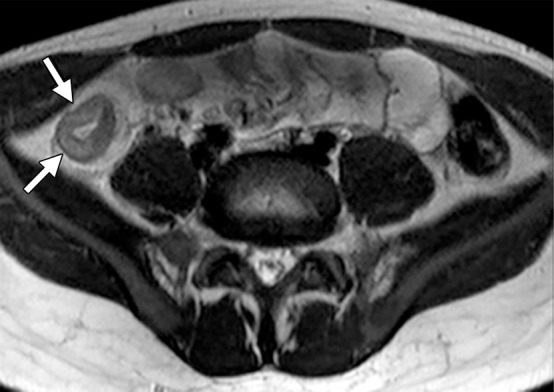
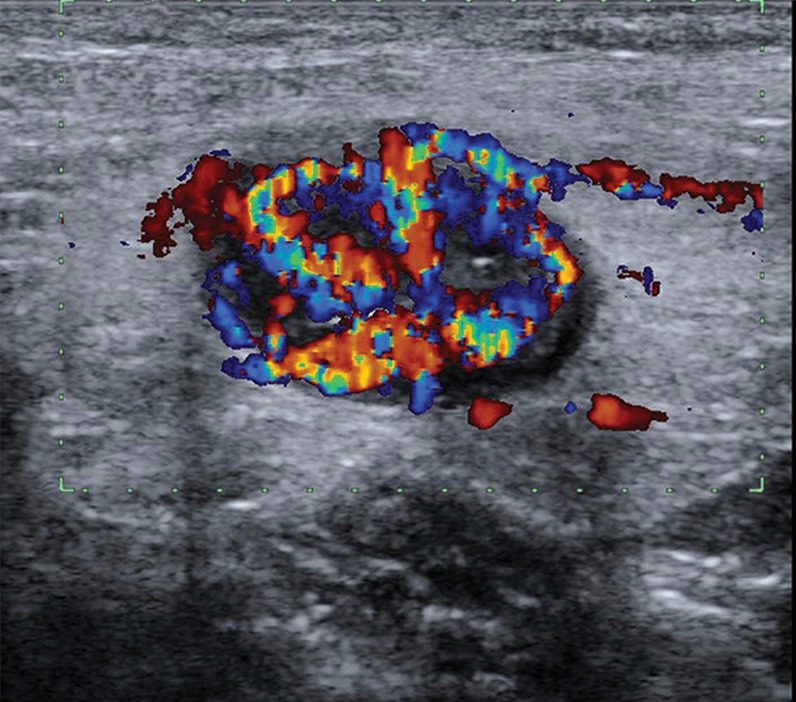
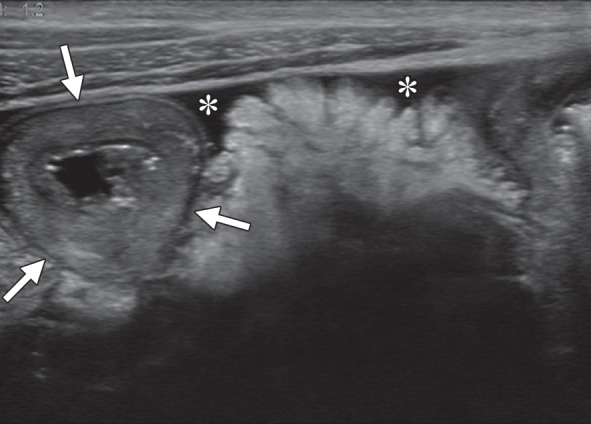
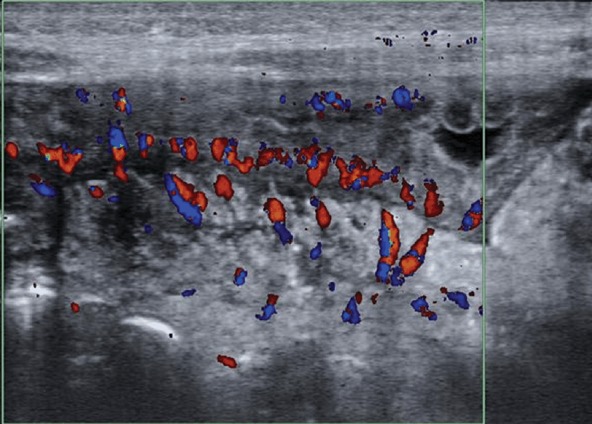
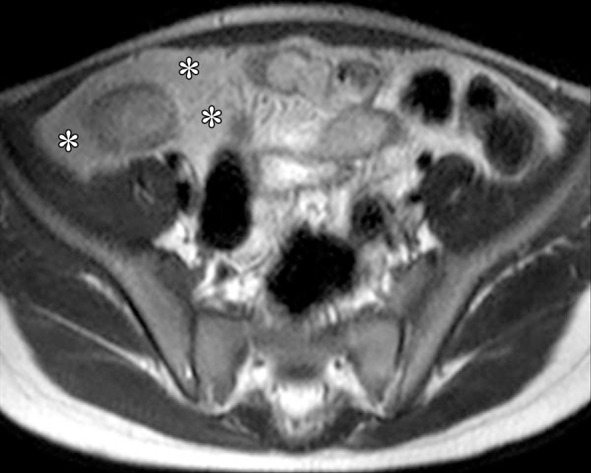
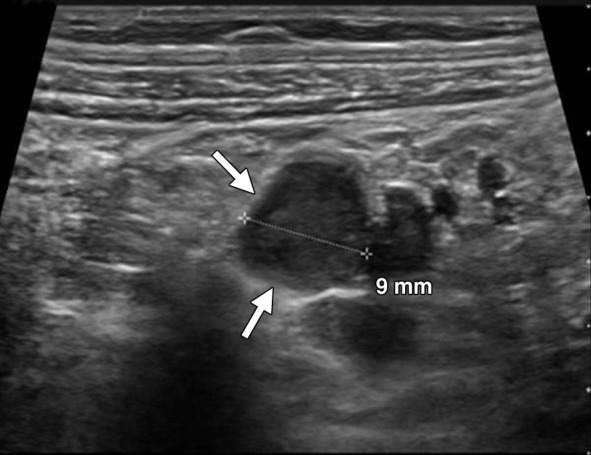
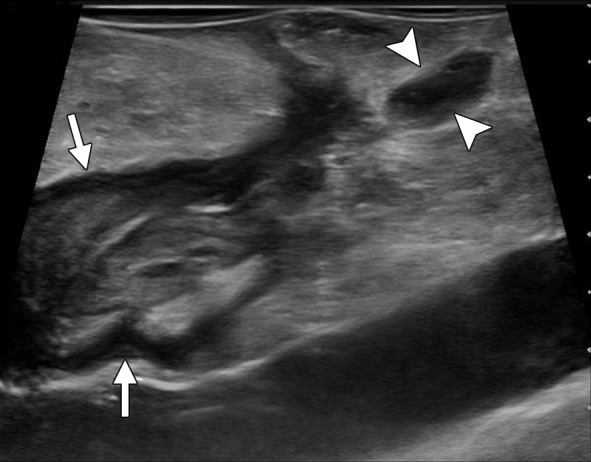
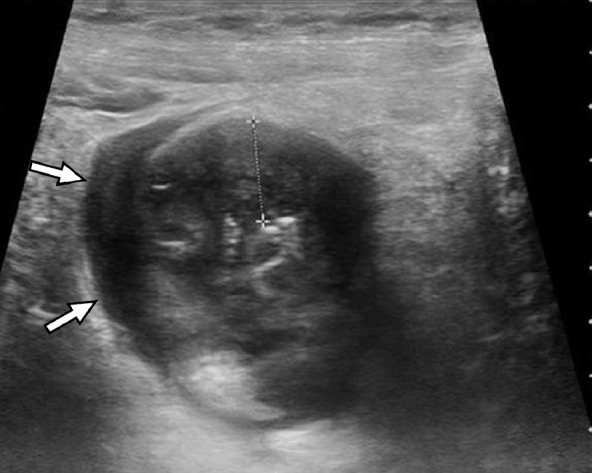
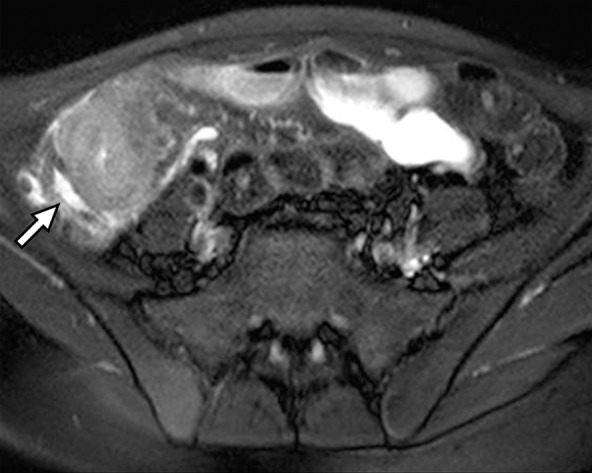
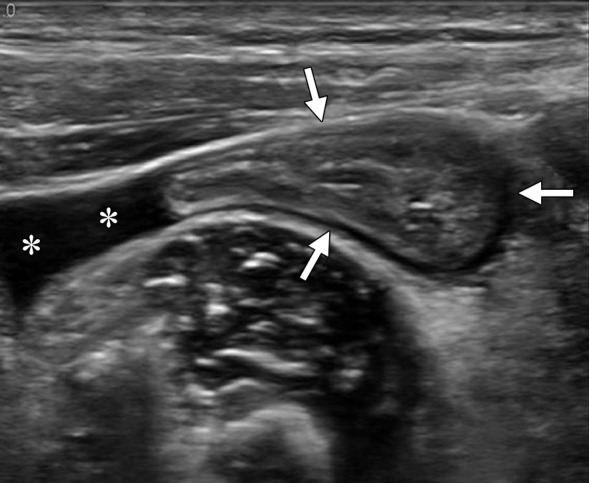
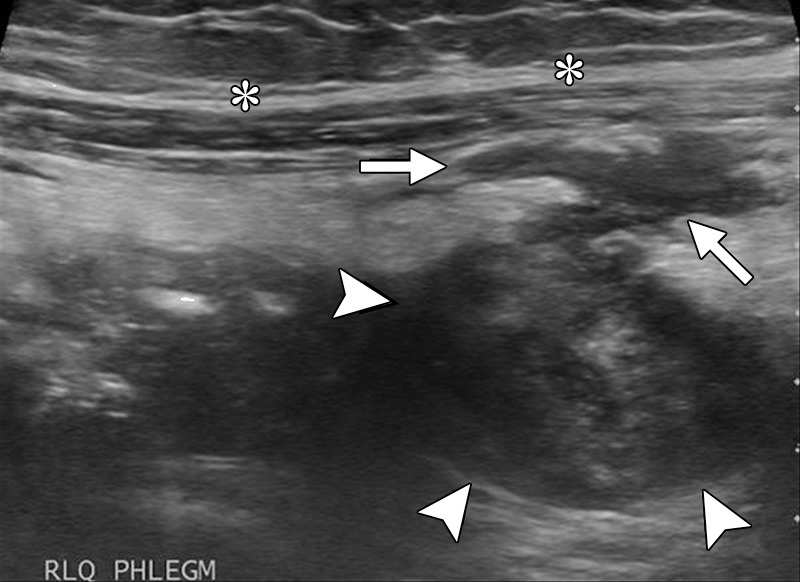
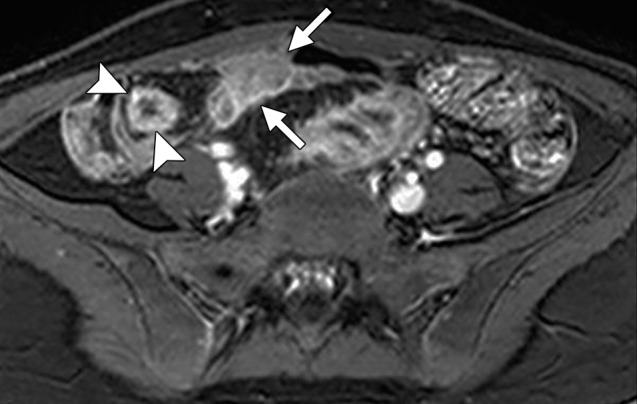
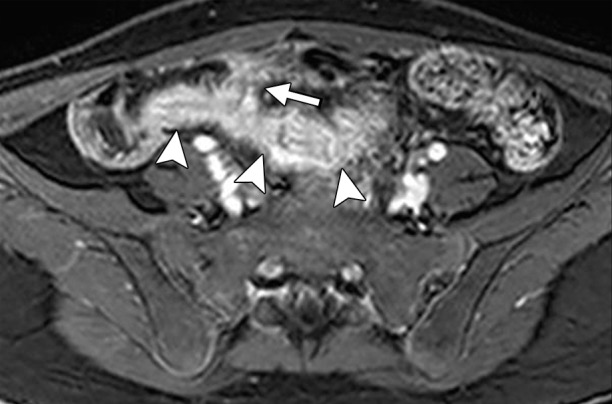
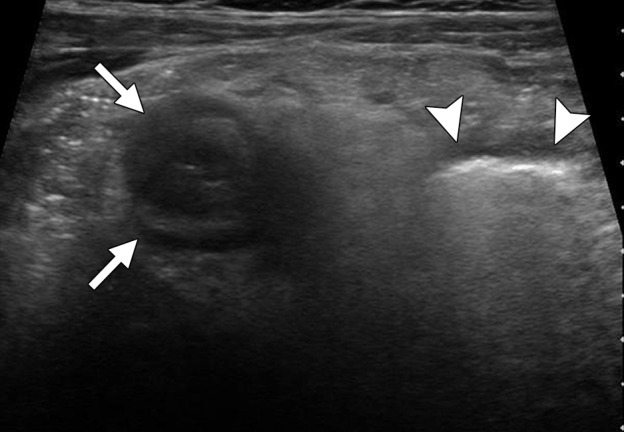
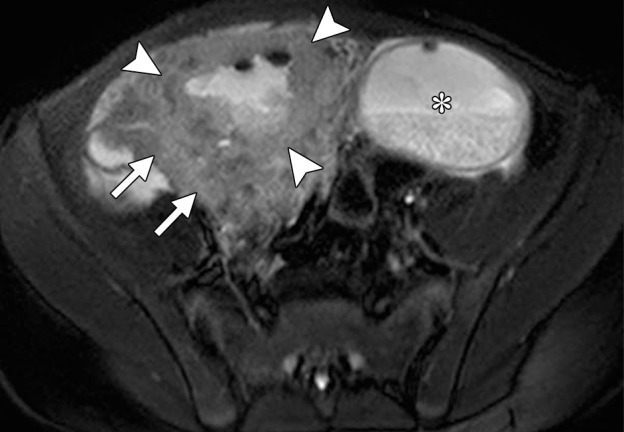
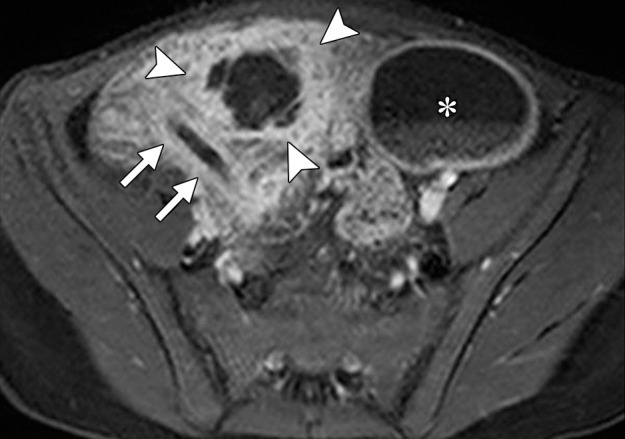
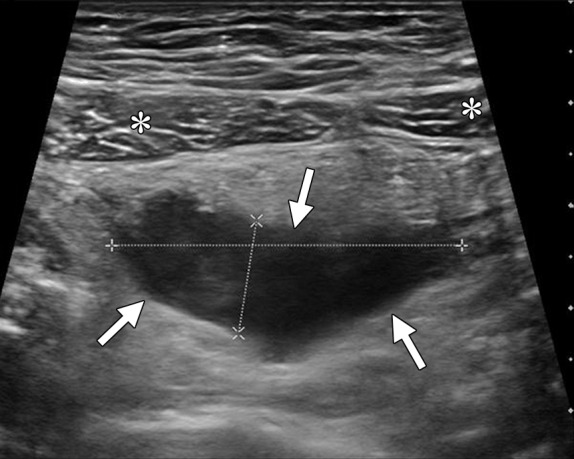
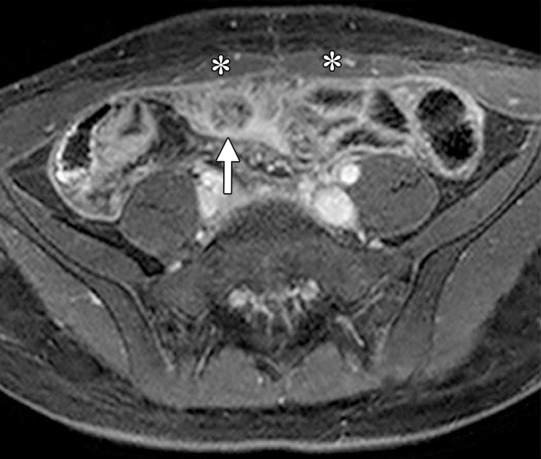
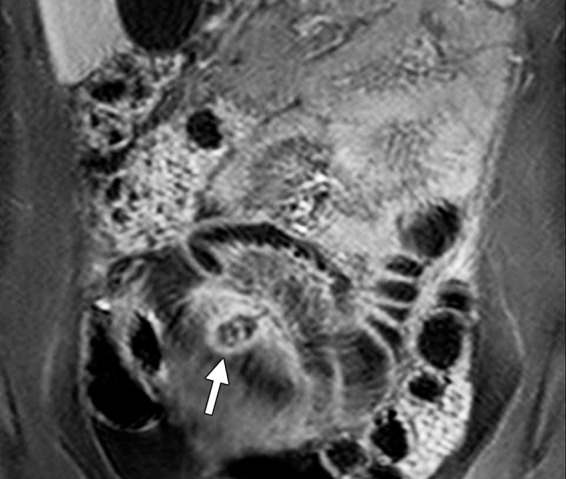
Small bowel Crohn disease is commonly diagnosed during the pediatric period, and recent investigations show that its incidence is increasing in this age group. Diagnosis and follow-up of this condition are commonly based on a combination of patient history and physical examination, disease activity surveys, laboratory assessment, and endoscopy with biopsy, but imaging also plays a central role. Ultrasonography (US) is an underutilized well-tolerated imaging modality for screening and follow-up of small bowel Crohn disease in children and adolescents. US has numerous advantages over computed tomographic (CT) enterography and magnetic resonance (MR) enterography, including low cost and no required use of oral or intravenous contrast material. US also has the potential to provide images with higher spatial resolution than those obtained at CT enterography and MR enterography, allows faster examination than does MR enterography, does not involve ionizing radiation, and does not require sedation or general anesthesia. US accurately depicts small bowel and mesenteric changes related to pediatric Crohn disease, and US findings show a high correlation with MR imaging findings in this patient population.
(©)RSNA, 2015.
Figures






References
-
- Yu AP, Cabanilla LA, Wu EQ, Mulani PM, Chao J. The costs of Crohn’s disease in the United States and other Western countries: a systematic review. Curr Med Res Opin 2008;24(2):319–328. - PubMed
-
- Benitez JM, Meuwis MA, Reenaers C, Van Kemseke C, Meunier P, Louis E. Role of endoscopy, cross-sectional imaging and biomarkers in Crohn’s disease monitoring. Gut 2013;62(12):1806–1816. - PubMed
-
- Domina JG, Dillman JR, Adler J, et al. Imaging trends and radiation exposure in pediatric inflammatory bowel disease at an academic children’s hospital. AJR Am J Roentgenol 2013;201(1):W133–W140. - PubMed
Publication types
MeSH terms
Substances
Supplementary concepts
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
