

Impact of National Cancer Institute Comprehensive Cancer Centers on ovarian cancer treatment and survival
- PMID: 25840536
- PMCID: PMC5145798
- DOI: 10.1016/j.jamcollsurg.2015.01.056
Impact of National Cancer Institute Comprehensive Cancer Centers on ovarian cancer treatment and survival
Abstract
Background: The regional impact of care at a National Cancer Institute Comprehensive Cancer Center (NCI-CCC) on adherence to National Comprehensive Cancer Network (NCCN) ovarian cancer treatment guidelines and survival is unclear.
Study design: We performed a retrospective population-based study of consecutive patients diagnosed with epithelial ovarian cancer between January 1, 1996 and December 31, 2006 in southern California. Patients were stratified according to care at an NCI-CCC (n = 5), non-NCI high-volume hospital (≥ 10 cases/year, HVH, n = 29), or low-volume hospital (<10 cases/year, LVH, n = 158). Multivariable logistic regression and Cox-proportional hazards models were used to examine the effect of NCI-CCC status on treatment guideline adherence and ovarian cancer-specific survival.
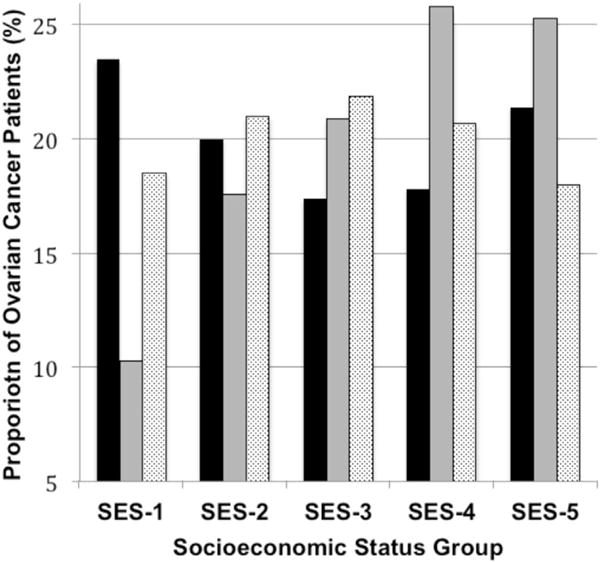
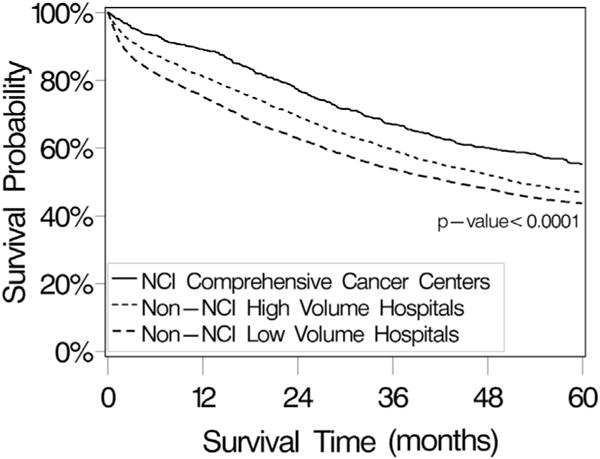
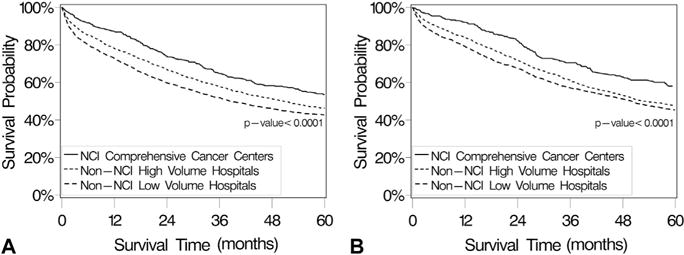
Results: A total of 9,933 patients were identified (stage I, 22.8%; stage II, 7.9%; stage III, 45.1%; stage IV, 24.2%), and 8.1% of patients were treated at NCI-CCCs. Overall, 35.7% of patients received NCCN guideline adherent care, and NCI-CCC status (odds ratio [OR] 1.00) was an independent predictor of adherence to treatment guidelines compared with HVHs (OR 0.83, 95% CI 0.70 to 0.99) and LVHs (OR 0.56, 95% CI 0.47 to 0.67). The median ovarian cancer-specific survivals according to hospital type were: NCI-CCC 77.9 (95% CI 61.4 to 92.9) months, HVH 51.9 (95% CI 49.2 to 55.7) months, and LVH 43.4 (95% CI 39.9 to 47.2) months (p < 0.0001). National Cancer Institute Comprehensive Cancer Center status (hazard ratio [HR] 1.00) was a statistically significant and independent predictor of improved survival compared with HVH (HR 1.18, 95% CI 1.04 to 1.33) and LVH (HR 1.30, 95% CI 1.15 to 1.47).
Conclusions: National Cancer Institute Comprehensive Cancer Center status is an independent predictor of adherence to ovarian cancer treatment guidelines and improved ovarian cancer-specific survival. These data validate NCI-CCC status as a structural health care characteristic correlated with superior ovarian cancer quality measure performance. Increased access to NCI-CCCs through regional concentration of care may be a mechanism to improve clinical outcomes.
Copyright © 2015 American College of Surgeons. Published by Elsevier Inc. All rights reserved.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics 2013. CA Cancer J Clin. 2013;63:11–30. - PubMed
-
- Bristow RE, Chang J, Ziogas A, et al. Adherence to treatment guidelines for ovarian cancer as a measure of quality care. Obstet Gynecol. 2013;121:1226–1234. - PubMed
-
- Read C, Elit L. Trends in gynecologic cancer care in North America. Obstet Gynecol Clin North Am. 2012;39:107–129. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
