

The Polycystic Ovary Morphology-Polycystic Ovary Syndrome Spectrum
- PMID: 25840648
- PMCID: PMC4387116
- DOI: 10.1016/j.jpag.2014.07.016
The Polycystic Ovary Morphology-Polycystic Ovary Syndrome Spectrum
Abstract
Background: Polycystic ovary syndrome (PCOS) is the most common cause of chronic hyperandrogenic anovulation. Two-thirds of PCOS patients have functionally typical PCOS, with typical functional ovarian hyperandrogenism manifest as 17-hydroxyprogesterone hyper-responsiveness to gonadotropin stimulation. Most, but not all, of the remainder have atypical functional ovarian hyperandrogenism. Many asymptomatic volunteers with polycystic ovary morphology (PCOM) have similar abnormalities.
Objective: The objective of this paper is to review the relationship of biochemical ovarian function to the clinical spectrum observed in PCOS and in normal volunteers with PCOM.
Findings: Adolescents and adults with PCOS are similar clinically and biochemically. Ninety-five percent of functionally typical PCOS have classic PCOS, ie, hyperandrogenic anovulation with PCOM. In addition to having more severe hyperandrogenism and a greater prevalence of PCOM than other PCOS, they have a significantly greater prevalence of glucose intolerance although insulin resistance is similarly reduced. Half of normal-variant PCOM have PCOS-related steroidogenic dysfunction, which suggests a PCOS carrier state.
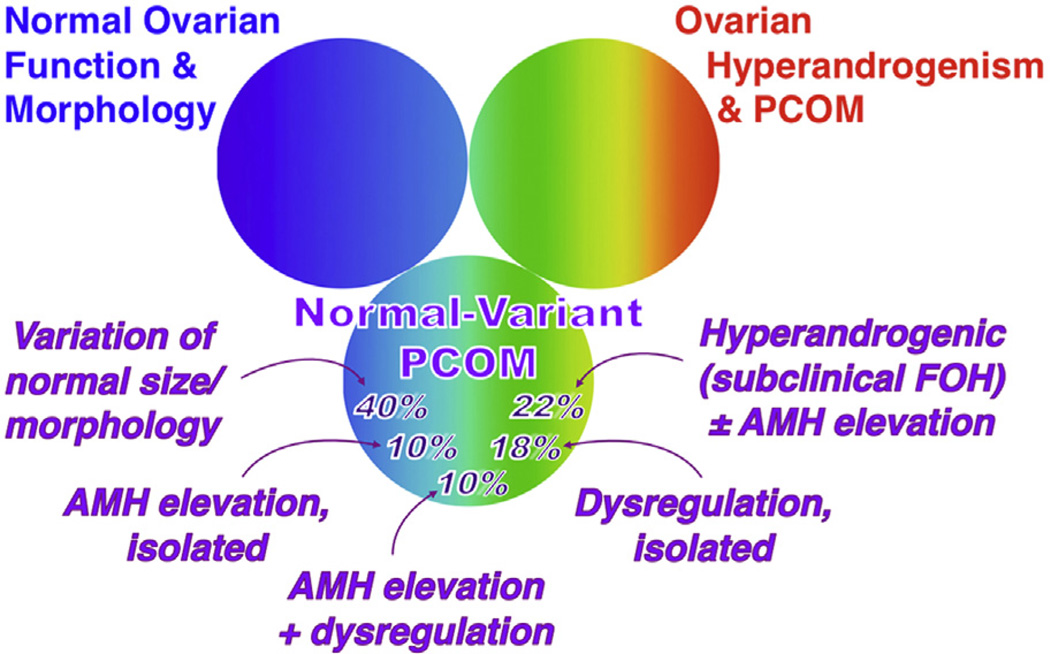
Conclusions: There is a spectrum of ovarian androgenic dysfunction that ranges from subclinical hyperandrogenemia in some normal-variant PCOM to severe ovarian hyperandrogenism in most classic PCOS. A minority of mild PCOS cases do not fall on this spectrum of ovarian androgenic dysfunction, but rather seem to have obesity as the basis of their hyperandrogenism, or, less often, isolated adrenal androgenic dysfunction. Half of normal-variant PCOM also do not fall on the PCOS spectrum, and some of these seem to have excessive folliculogenesis as a variant that may confer mild prolongation of the reproductive lifespan. Improved understanding of PCOM in young women is needed.
Keywords: Glucose intolerance; Insulin resistance; Obesity; Polycystic ovary; Polycystic ovary syndrome.
Copyright © 2015 North American Society for Pediatric and Adolescent Gynecology. Published by Elsevier Inc. All rights reserved.
Conflict of interest statement
The authors indicate no conflicts of interest.
Figures


Comment in
-
Polycystic Ovarian Syndrome Since Stein and Leventhal.J Pediatr Adolesc Gynecol. 2015 Dec;28(6):411. doi: 10.1016/j.jpag.2015.10.001. Epub 2015 Oct 9. J Pediatr Adolesc Gynecol. 2015. PMID: 26456202 No abstract available.
References
-
- Azziz R, Sanchez LA, Knochenhauer ES, et al. Androgen excess in women: experience with over 1000 consecutive patients. J Clin Endocrinol Metab. 2004;89:453. - PubMed
-
- Carmina E, Rosato F, Janni A, et al. Extensive clinical experience: relative prevalence of different androgen excess disorders in 950 women referred because of clinical hyperandrogenism. J Clin Endocrinol Metab. 2006;91:2. - PubMed
-
- Ehrmann DA, Barnes RB, Rosenfield RL. Polycystic ovary syndrome as a form of functional ovarian hyperandrogenism due to dysregulation of androgen secretion. Endocr Rev. 1995;16:322. - PubMed
-
- Rosenfield RL. Clinical review: Identifying children at risk of polycystic ovary syndrome. J Clin Endocrinol Metab. 2007;92:787. - PubMed
-
- Franks S. Polycystic ovary syndrome in adolescents. Int J Obes (Lond) 2008;32:1035. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
