

Circulating tumour DNA and CT monitoring in patients with untreated diffuse large B-cell lymphoma: a correlative biomarker study
- PMID: 25842160
- PMCID: PMC4460610
- DOI: 10.1016/S1470-2045(15)70106-3
Circulating tumour DNA and CT monitoring in patients with untreated diffuse large B-cell lymphoma: a correlative biomarker study
Erratum in
-
Correction to Lancet Oncol 2015; 16: 545.Lancet Oncol. 2015 May;16(5):e199. doi: 10.1016/S1470-2045(15)70217-2. Lancet Oncol. 2015. PMID: 25943062 No abstract available.
Abstract
Background: Diffuse large-B-cell lymphoma is curable, but when treatment fails, outcome is poor. Although imaging can help to identify patients at risk of treatment failure, they are often imprecise, and radiation exposure is a potential health risk. We aimed to assess whether circulating tumour DNA encoding the clonal immunoglobulin gene sequence could be detected in the serum of patients with diffuse large-B-cell lymphoma and used to predict clinical disease recurrence after frontline treatment.
Methods: We used next-generation DNA sequencing to retrospectively analyse cell-free circulating tumour DNA in patients assigned to one of three treatment protocols between May 8, 1993, and June 6, 2013. Eligible patients had diffuse large-B-cell lymphoma, no evidence of indolent lymphoma, and were previously untreated. We obtained serial serum samples and concurrent CT scans at specified times during most treatment cycles and up to 5 years of follow-up. VDJ gene segments of the rearranged immunoglobulin receptor genes were amplified and sequenced from pretreatment specimens and serum circulating tumour DNA encoding the VDJ rearrangements was quantitated.
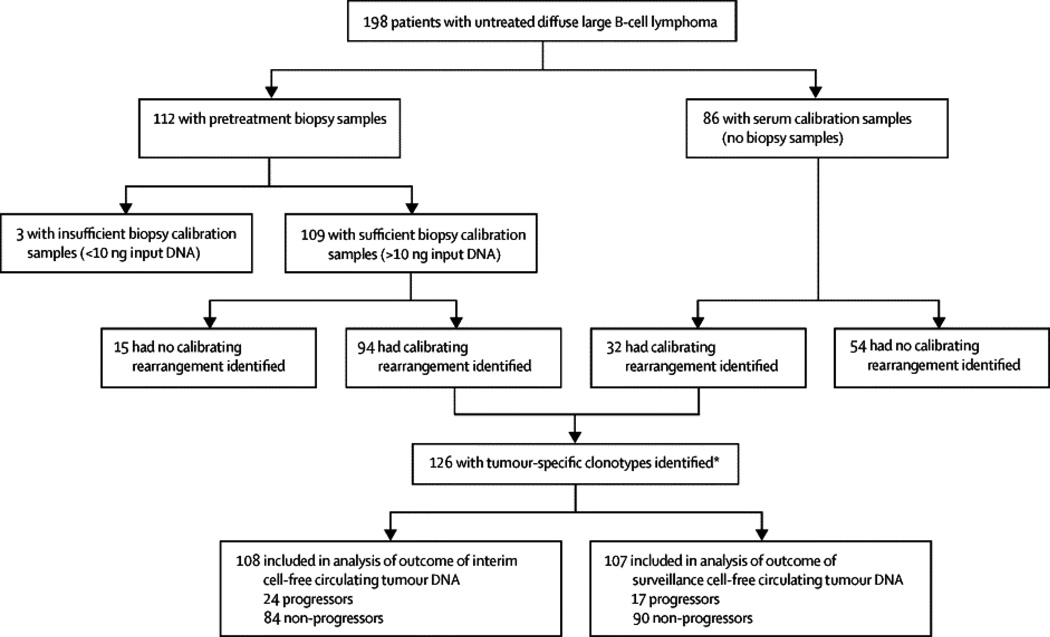
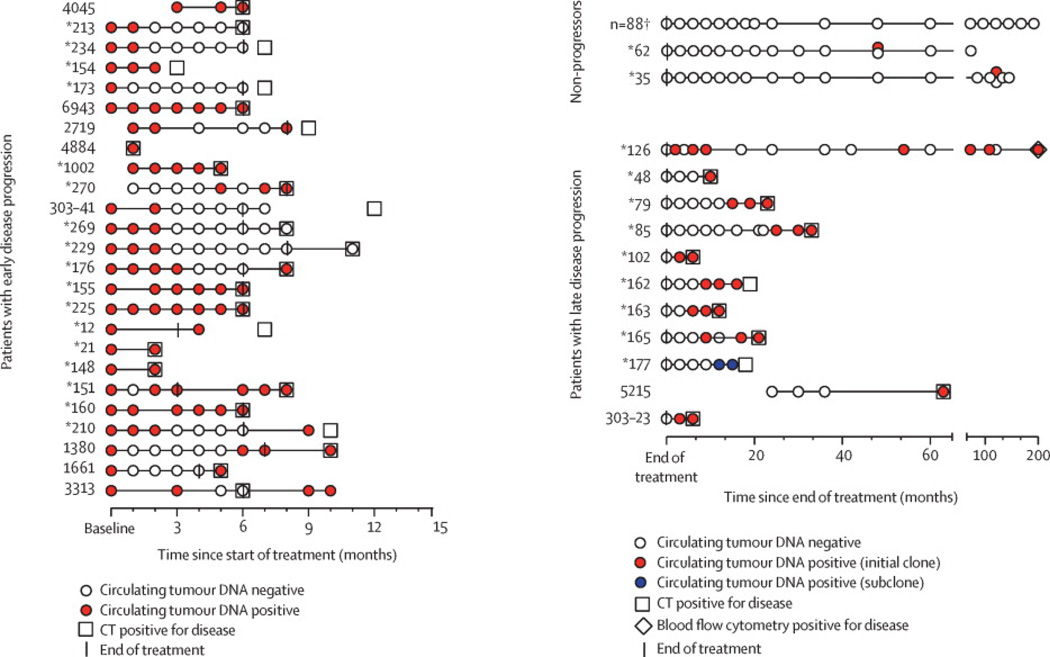
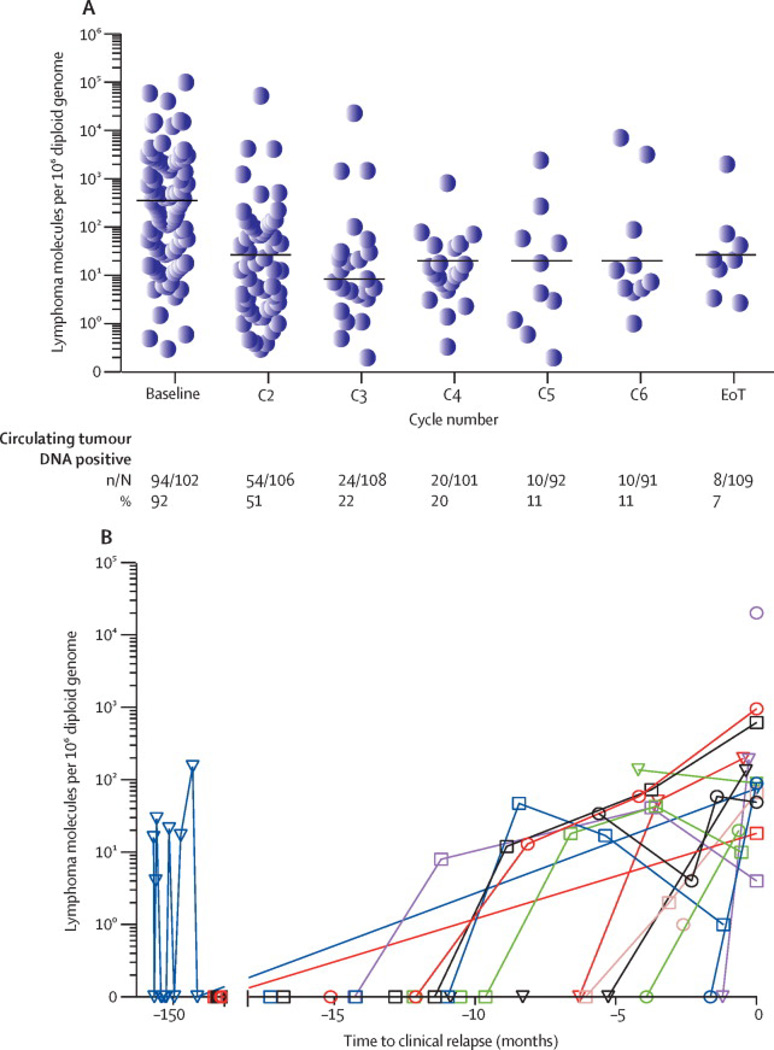
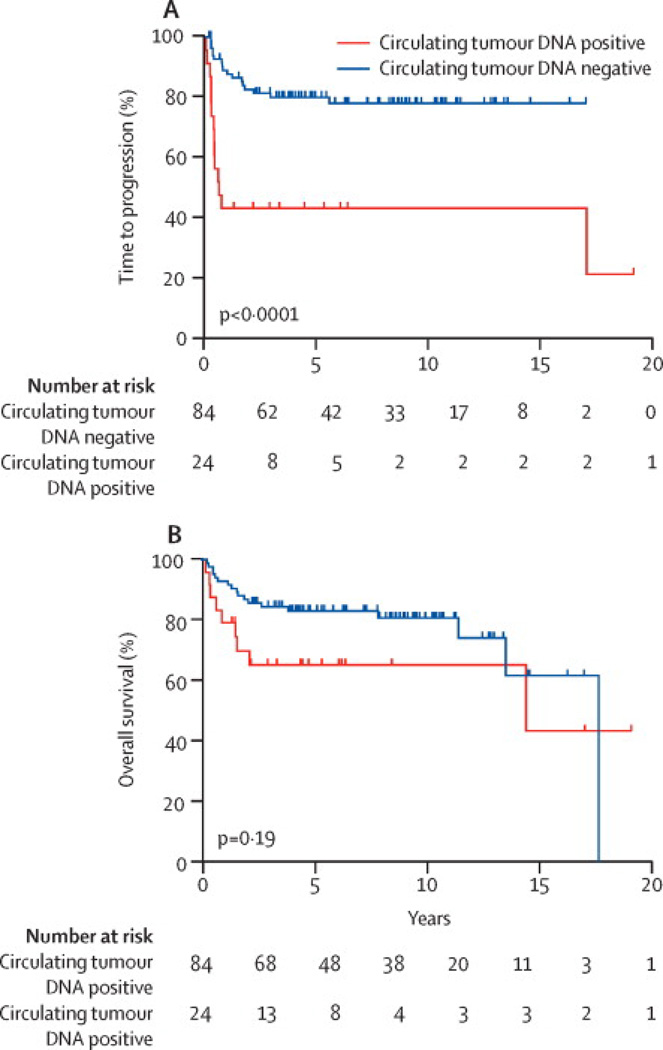
Findings: Tumour clonotypes were identified in pretreatment specimens from 126 patients who were followed up for a median of 11 years (IQR 6·8-14·2). Interim monitoring of circulating tumour DNA at the end of two treatment cycles in 108 patients showed a 5-year time to progression of 41·7% (95% CI 22·2-60·1) in patients with detectable circulating tumour DNA and 80·2% (69·6-87·3) in those without detectable circulating tumour DNA (p<0·0001). Detectable interim circulating tumour DNA had a positive predictive value of 62·5% (95% CI 40·6-81·2) and a negative predictive value of 79·8% (69·6-87·8). Surveillance monitoring of circulating tumour DNA was done in 107 patients who achieved complete remission. A Cox proportional hazards model showed that the hazard ratio for clinical disease progression was 228 (95% CI 51-1022) for patients who developed detectable circulating tumour DNA during surveillance compared with patients with undetectable circulating tumour DNA (p<0·0001). Surveillance circulating tumour DNA had a positive predictive value of 88·2% (95% CI 63·6-98·5) and a negative predictive value of 97·8% (92·2-99·7) and identified risk of recurrence at a median of 3·5 months (range 0-200) before evidence of clinical disease.
Interpretation: Surveillance circulating tumour DNA identifies patients at risk of recurrence before clinical evidence of disease in most patients and results in a reduced disease burden at relapse. Interim circulating tumour DNA is a promising biomarker to identify patients at high risk of treatment failure.
Funding: National Cancer Institute and Adaptive Biotechnologies.
Copyright © 2015 Elsevier Ltd. All rights reserved.
Conflict of interest statement
DECLARATION OF INTEREST
MR, KD, SP, MS, ESJ, LMS, CL, SMS, CCC and WHW have no conflicts to declare.
Figures
Comment in
-
Large B-cell lymphoma: is the future written in the blood?Lancet Oncol. 2015 May;16(5):481-3. doi: 10.1016/S1470-2045(15)70160-9. Epub 2015 Apr 1. Lancet Oncol. 2015. PMID: 25842159 No abstract available.
-
Biomarkers: ctDNA-identifying cancer before it is clinically detectable.Nat Rev Clin Oncol. 2015 Jul;12(7):372. doi: 10.1038/nrclinonc.2015.77. Epub 2015 Apr 21. Nat Rev Clin Oncol. 2015. PMID: 25895612 No abstract available.
References
-
- Liedtke M, Hamlin PA, Moskowitz CH, Zelenetz AD. Surveillance imaging during remission identifies a group of patients with more favorable aggressive NHL at time of relapse: a retrospective analysis of a uniformly-treated patient population. Ann Oncol. 2006;17(6):909–913. - PubMed
-
- Armitage JO. Who benefits from surveillance imaging? J Clin Oncol. 2012;30(21):2579–2580. - PubMed
Publication types
MeSH terms
Substances
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
