

Surgery versus nonsurgical treatment of lumbar spinal stenosis: a randomized trial
- PMID: 25844995
- PMCID: PMC6252248
- DOI: 10.7326/M14-1420
Surgery versus nonsurgical treatment of lumbar spinal stenosis: a randomized trial
Abstract
Background: Primary care management decisions for patients with symptomatic lumbar spinal stenosis (LSS) are challenging, and nonsurgical guidance is limited by lack of evidence.
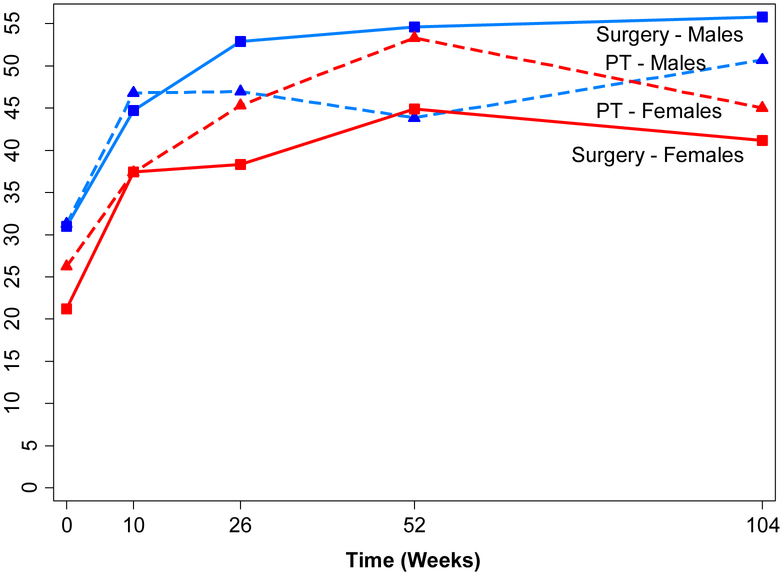
Objective: To compare surgical decompression with physical therapy (PT) for LSS and evaluate sex differences.
Design: Multisite randomized, controlled trial. (ClinicalTrials.gov: NCT00022776).
Setting: Neurologic and orthopedic surgery departments and PT clinics.
Participants: Surgical candidates with LSS aged 50 years or older who consented to surgery.
Intervention: Surgical decompression or PT.
Measurements: Primary outcome was physical function score on the Short Form-36 Health Survey at 2 years assessed by masked testers.
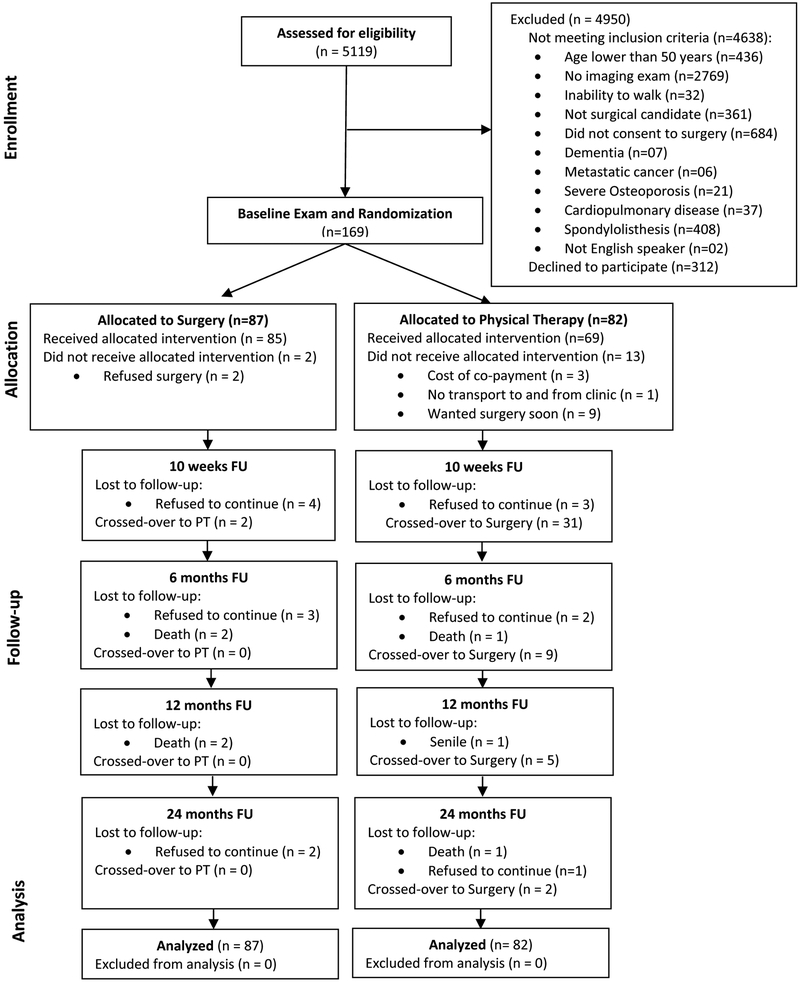
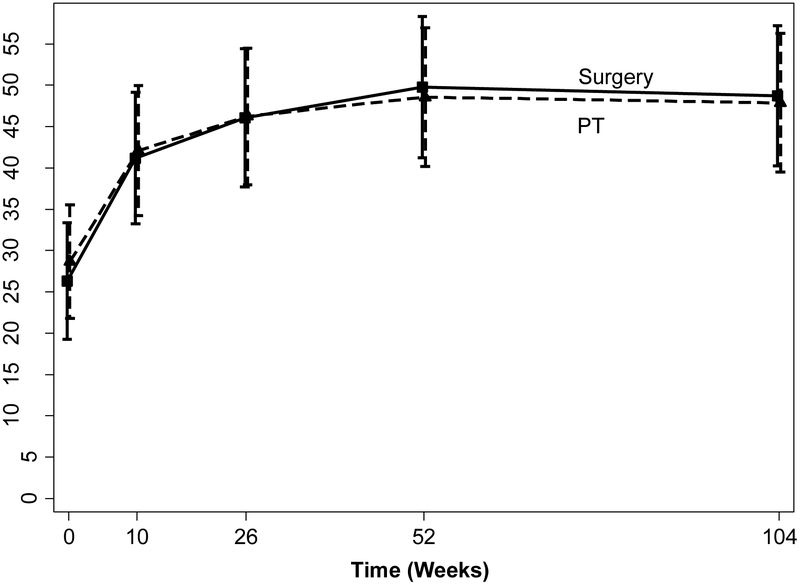
Results: The study took place from November 2000 to September 2007. A total of 169 participants were randomly assigned and stratified by surgeon and sex (87 to surgery and 82 to PT), with 24-month follow-up completed by 74 and 73 participants in the surgery and PT groups, respectively. Mean improvement in physical function for the surgery and PT groups was 22.4 (95% CI, 16.9 to 27.9) and 19.2 (CI, 13.6 to 24.8), respectively. Intention-to-treat analyses revealed no difference between groups (24-month difference, 0.9 [CI, -7.9 to 9.6]). Sensitivity analyses using causal-effects methods to account for the high proportion of crossovers from PT to surgery (57%) showed no significant differences in physical function between groups.
Limitation: Without a control group, it is not possible to judge success attributable to either intervention.
Conclusion: Surgical decompression yielded similar effects to a PT regimen among patients with LSS who were surgical candidates. Patients and health care providers should engage in shared decision-making conversations that include full disclosure of evidence involving surgical and nonsurgical treatments for LSS.
Primary funding source: National Institutes of Health and National Institute of Arthritis and Musculoskeletal and Skin Diseases.
Figures
Comment in
-
Surgery for lumbar spinal stenosis: informed patient preferences should weigh heavily.Ann Intern Med. 2015 Apr 7;162(7):518-9. doi: 10.7326/M15-0360. Ann Intern Med. 2015. PMID: 25844999 No abstract available.
-
Physical therapy is as effective as surgery for lumbar spinal stenosis, study finds.BMJ. 2015 Apr 6;350:h1827. doi: 10.1136/bmj.h1827. BMJ. 2015. PMID: 25852064 No abstract available.
-
Surgery Versus Nonsurgical Treatment of Lumbar Spinal Stenosis.Ann Intern Med. 2015 Sep 1;163(5):396. doi: 10.7326/L15-5129. Ann Intern Med. 2015. PMID: 26322700 No abstract available.
-
Surgery Versus Nonsurgical Treatment of Lumbar Spinal Stenosis.Ann Intern Med. 2015 Sep 1;163(5):396-7. doi: 10.7326/L15-5129-2. Ann Intern Med. 2015. PMID: 26322701 No abstract available.
-
Surgery Versus Nonsurgical Treatment of Lumbar Spinal Stenosis.Ann Intern Med. 2015 Sep 1;163(5):397. doi: 10.7326/L15-5129-3. Ann Intern Med. 2015. PMID: 26322702 No abstract available.
-
Surgery Versus Nonsurgical Treatment of Lumbar Spinal Stenosis.Ann Intern Med. 2015 Sep 1;163(5):397-8. doi: 10.7326/L15-5129-4. Ann Intern Med. 2015. PMID: 26322703 Free PMC article. No abstract available.
-
No differences between physiotherapy and decompression surgery for patients considered surgical candidates for lumbar spinal stenosis [synopsis].J Physiother. 2016 Jan;62(1):49. doi: 10.1016/j.jphys.2015.09.003. Epub 2015 Dec 11. J Physiother. 2016. PMID: 26701158 No abstract available.
-
No differences between physiotherapy and decompression surgery for patients considered surgical candidates for lumbar spinal stenosis [commentary].J Physiother. 2016 Jan;62(1):49. doi: 10.1016/j.jphys.2015.09.005. Epub 2015 Dec 11. J Physiother. 2016. PMID: 26701160 No abstract available.
-
Surgery and physical therapy likely yield similar outcomes in spinal stenosis.Evid Based Med. 2016 Feb;21(1):31. doi: 10.1136/ebmed-2015-110220. Epub 2016 Jan 4. Evid Based Med. 2016. PMID: 26729775 No abstract available.
References
-
- Katz JN, Harris MB. Clinical practice. Lumbar spinal stenosis. [Review] [44 refs]. New England Journal of Medicine. 2008;358(8):818–25. - PubMed
-
- Boden SD. The use of radiographic imaging studies in the evaluation of patients who have degenerative disorders of the lumbar spine. [Review] [128 refs]. Journal of Bone & Joint Surgery - American Volume. 1996;78(1):114–24. - PubMed
-
- Katz JN, Dalgas M, Stucki G, Katz NP, Bayley J, Fossel AH, et al. Degenerative lumbar spinal stenosis. Diagnostic value of the history and physical examination. Arthritis & Rheumatism. 1995;38(9):1236–41. - PubMed
-
- Deyo RA. Treatment of lumbar spinal stenosis: a balancing act. Spine Journal: Official Journal of the North American Spine Society. 2010;10(7):625–7. - PubMed
-
- Atlas SJ, Delitto A. Spinal stenosis: surgical versus nonsurgical treatment. [Review] [92 refs]. Clinical Orthopaedics & Related Research. 2006;443:198–207. - PubMed
Publication types
MeSH terms
Associated data
Grants and funding
LinkOut - more resources
Full Text Sources
Medical