

Does Combined Intra- and Extraarticular ACL Reconstruction Improve Function and Stability? A Meta-analysis
- PMID: 25845949
- PMCID: PMC4488196
- DOI: 10.1007/s11999-015-4285-y
Does Combined Intra- and Extraarticular ACL Reconstruction Improve Function and Stability? A Meta-analysis
Abstract
Background: ACL reconstruction aims to restore knee function and stability; however, rotational stability may not be completely restored by use of standard intraarticular reconstruction alone. Although individual studies have not shown the superiority of combined ACL reconstruction compared with isolated intraarticular reconstruction in terms of function and stability, biomechanical principles suggest a combined approach may be helpful, therefore pooling (meta-analyzing) the available randomized clinical studies may be enlightening.
Questions/purposes: We performed a meta-analysis to determine whether combining extraarticular with intraarticular ACL reconstruction would lead to: (1) similar knee function measured by the IKDC evaluation, return-to-activity, and Tegner Lysholm scores, compared with isolated intraarticular reconstruction; (2) increased stability measured by pivot shift and instrumented Lachman examination; and (3) any differences in complications and adverse events?
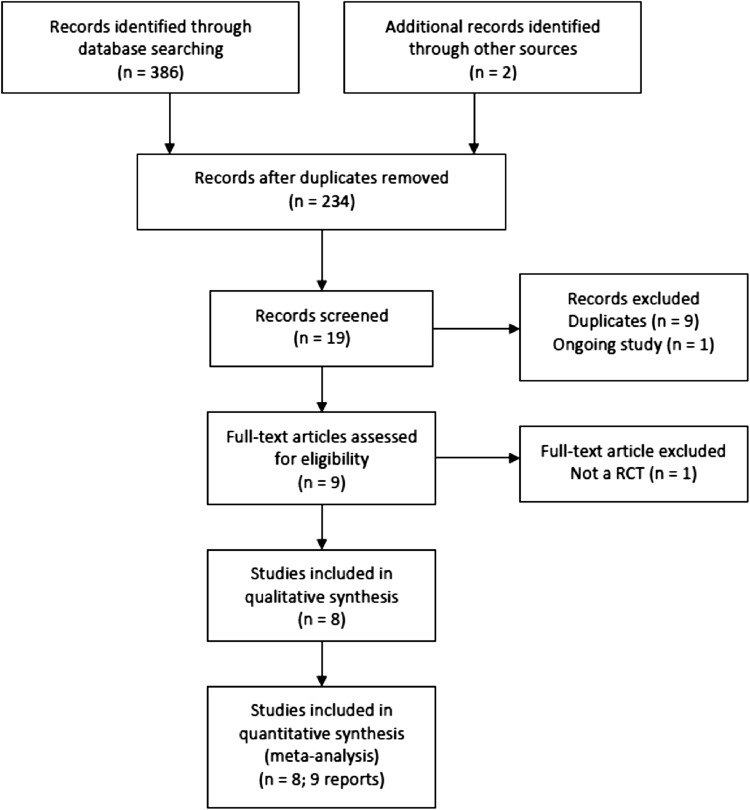
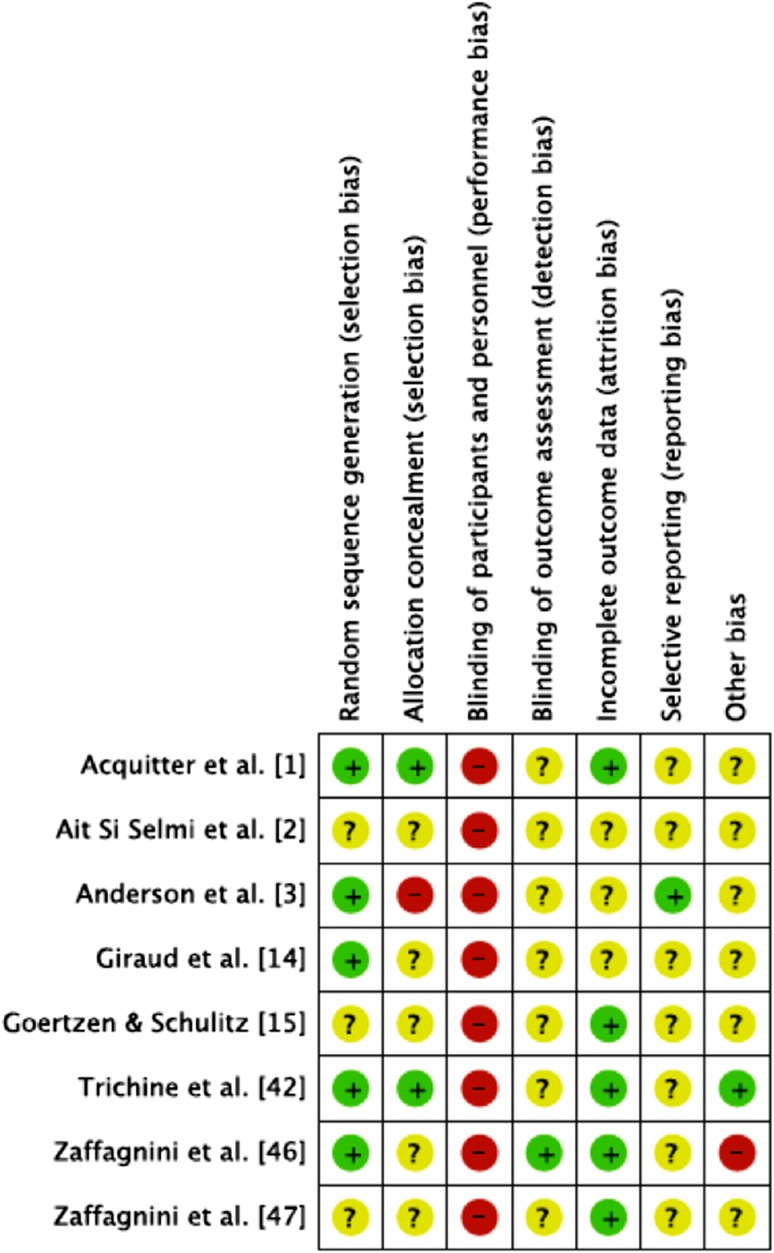
Methods: To identify randomized controlled trials (RCTs) comparing combined intra- and extrarticular ACL reconstruction (combined reconstruction) with intraarticular ACL reconstruction only, we searched MEDLINE, EMBASE, SPORTDiscus, Latin American and Caribbean Health Sciences (LILACS), and the Cochrane Central Register of Controlled Trials, and followed the Preferred Reporting Items for Systematic Reviews and Meta-Analyses (PRISMA) criteria. The main outcomes we sought were patient function and stability and complications after ACL reconstruction. Of 386 identified studies, eight RCTs were included (n=682 participants; followup, 12-84 months; men to women ratio, 2.17:1) in our meta-analysis. Study quality (internal validity) was assessed using the Cochrane risk-of-bias tool; in general, we found a moderate quality of evidence of the included studies.
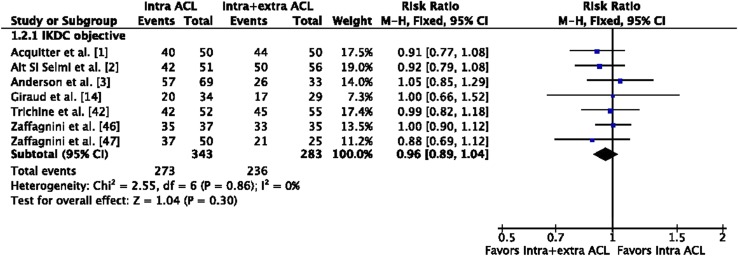
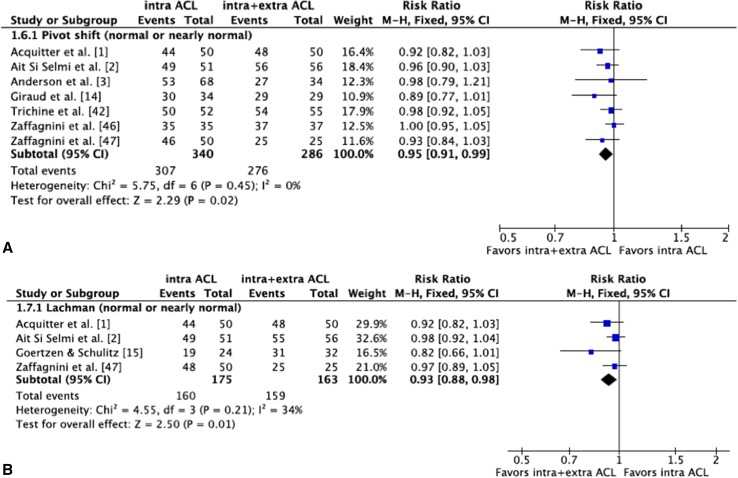
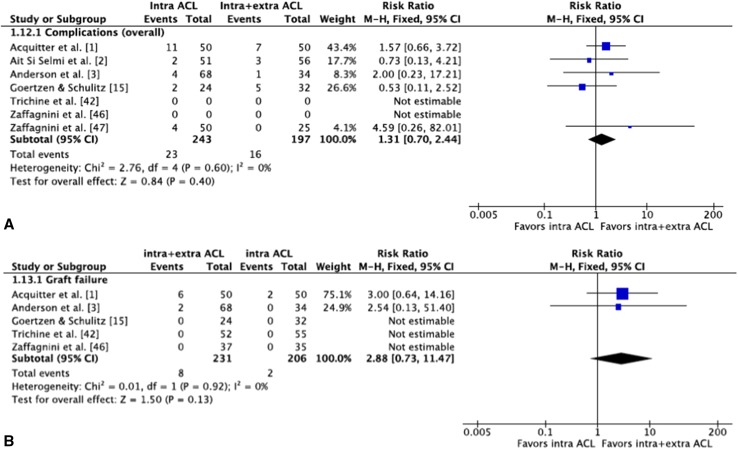
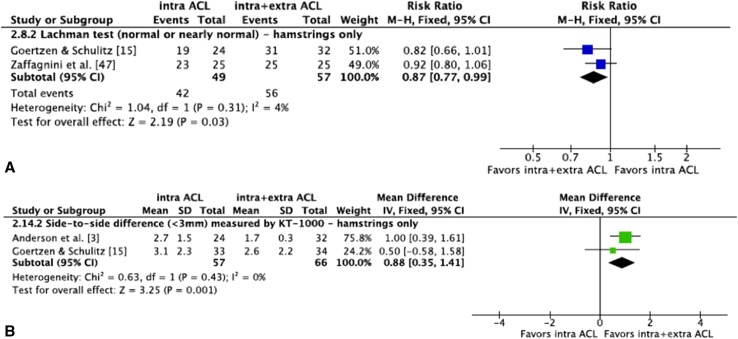
Results: When functional outcomes were compared, we found no difference between patients who underwent intraarticular ACL reconstruction only and those who underwent combined reconstruction (IKDC, return-to-activity, and Tegner Lysholm scores). However, patients who underwent combined reconstruction were more likely to show improved stability based on the pivot shift test (risk ratio [RR], 0.95; 95% CI, 0.91-0.99; p=0.02) and Lachman test (RR, 0.93; 95% CI, 0.88-0.98; p=0.01). In addition, our meta-analysis found no difference between the two treatments in terms of general complications or adverse events (RR, 1.31; 95% CI, 0.70-2.34; p=0.40) and the proportion of patients whose reconstructions failed (RR, 2.88; 95% CI, 0.73-11.47; p=0.13).
Conclusion: Combined intra- and extraarticular ACL reconstruction provided marginally improved knee stability and comparable failure rates but no difference in patient-reported functional outcomes scores. Complications and adverse events such as knee stiffness may be underreported and technical factors such as graft placement were difficult to evaluate. Future studies are needed to determine whether the small differences in additional stability warrant the potential morbidity of the additional extraarticular procedure and to determine long-term failure rates.
Figures
Comment in
-
CORR Insights®: Does Combined Intra- and Extraarticular ACL Reconstruction Improve Function and Stability? A Meta-analysis.Clin Orthop Relat Res. 2015 Aug;473(8):2619-20. doi: 10.1007/s11999-015-4339-1. Epub 2015 May 27. Clin Orthop Relat Res. 2015. PMID: 26013148 Free PMC article. No abstract available.
Similar articles
-
Surgical intra- and extra-articular anterior cruciate ligament reconstruction: a meta-analysis.BMC Musculoskelet Disord. 2020 Jun 30;21(1):414. doi: 10.1186/s12891-020-03438-4. BMC Musculoskelet Disord. 2020. PMID: 32605641 Free PMC article.
-
Does sequence of graft tensioning affect outcomes in combined anterior and posterior cruciate ligament reconstructions?Clin Orthop Relat Res. 2015 Jan;473(1):235-43. doi: 10.1007/s11999-014-3939-5. Epub 2014 Sep 16. Clin Orthop Relat Res. 2015. PMID: 25224821 Free PMC article.
-
Outcomes of anterior cruciate ligament reconstruction using single-bundle versus double-bundle technique: meta-analysis of 19 randomized controlled trials.Arthroscopy. 2013 Feb;29(2):357-65. doi: 10.1016/j.arthro.2012.08.024. Arthroscopy. 2013. PMID: 23369481
-
Effects of pre-operative knee laxity on clinical outcomes after partial anterior cruciate ligament reconstruction.Knee. 2018 Jun;25(3):445-452. doi: 10.1016/j.knee.2018.02.012. Epub 2018 Apr 21. Knee. 2018. PMID: 29685502
-
Single-bundle versus double-bundle autologous anterior cruciate ligament reconstruction: a meta-analysis of randomized controlled trials at 5-year minimum follow-up.J Orthop Surg Res. 2018 Mar 10;13(1):50. doi: 10.1186/s13018-018-0753-x. J Orthop Surg Res. 2018. PMID: 29523208 Free PMC article. Review.
Cited by
-
Anatomic and Histological Study of the Anterolateral Aspect of the Knee: A SANTI Group Investigation.Orthop J Sports Med. 2018 Oct 11;6(10):2325967118799970. doi: 10.1177/2325967118799970. eCollection 2018 Oct. Orthop J Sports Med. 2018. PMID: 30345320 Free PMC article.
-
Combined reconstruction of the anterolateral ligament in chronic ACL injuries leads to better clinical outcomes than isolated ACL reconstruction.Knee Surg Sports Traumatol Arthrosc. 2018 Dec;26(12):3652-3659. doi: 10.1007/s00167-018-4934-2. Epub 2018 Apr 2. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 29610972
-
Clinical outcomes of extra-articular tenodesis/anterolateral reconstruction in the ACL injured knee.Knee Surg Sports Traumatol Arthrosc. 2018 Feb;26(2):596-604. doi: 10.1007/s00167-017-4596-5. Epub 2017 Jun 12. Knee Surg Sports Traumatol Arthrosc. 2018. PMID: 28608009 Review.
-
Clinical Results of Lateral Extra-Articular Tenodesis.Tech Orthop. 2018 Dec;33(4):232-238. doi: 10.1097/BTO.0000000000000309. Epub 2017 Dec 25. Tech Orthop. 2018. PMID: 30542222 Free PMC article.
-
Knee instability scores for ACL reconstruction.Curr Rev Musculoskelet Med. 2016 Jun;9(2):170-7. doi: 10.1007/s12178-016-9339-6. Curr Rev Musculoskelet Med. 2016. PMID: 26980119 Free PMC article. Review.
References
-
- Acquitter Y, Hulet C, Locker B, Delbarre JC, Jambou S, Vielpeau C. [Patellar tendon-bone autograft reconstruction of the anterior cruciate ligament for advanced-stage chronic anterior laxity: is an extra-articular plasty necessary? A prospective randomized study of 100 patients with five-year follow-up] [In French] Rev Chir Orthop Reparatrice Appar Mot. 2003;89:413–422. - PubMed
-
- Ait Si Selmi T, Fabie F, Massouh T, Adeleine P, Neyret P. Greffe du LCA au tendon rotulien sous arthroscopie avec ou sans plastie antéro-externe: etude prospective randomisée à propos de 120 cas. In: Chambat P, Neyret P, Deschamps G et al., eds. Le Genou du Sportif. Montpellier, France: Sauramps Medical; 2002:221.
-
- Anderson AF, Snyder RB, Lipscomb AB., Jr Anterior cruciate ligament reconstruction: a prospective randomized study of three surgical methods. Am J Sports Med. 2001;29:272–279. - PubMed
-
- Bull AM, Amis AA. The pivot-shift phenomenon: a clinical and biomechanical perspective. Knee. 1998;5:141–158. doi: 10.1016/S0968-0160(97)10027-8. - DOI
Publication types
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
