

Multidetector computed tomography pulmonary angiography in childhood acute pulmonary embolism
- PMID: 25846076
- PMCID: PMC4553120
- DOI: 10.1007/s00247-015-3336-6
Multidetector computed tomography pulmonary angiography in childhood acute pulmonary embolism
Abstract
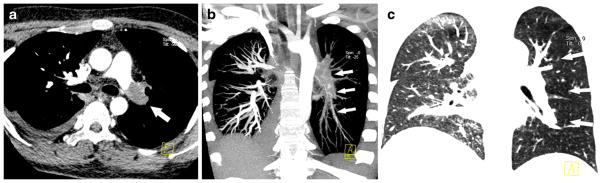
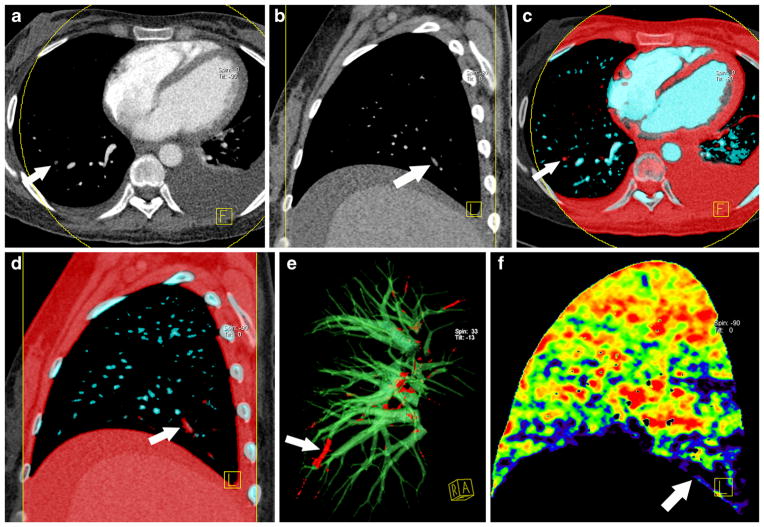
Pulmonary embolism is a life-threatening condition affecting people of all ages. Multidetector row CT pulmonary angiography has improved the imaging of pulmonary embolism in both adults and children and is now regarded as the routine modality for detection of pulmonary embolism. Advanced CT pulmonary angiography techniques developed in recent years, such as dual-energy CT, have been applied as a one-stop modality for pulmonary embolism diagnosis in children, as they can simultaneously provide anatomical and functional information. We discuss CT pulmonary angiography techniques, common and uncommon findings of pulmonary embolism in both conventional and dual-energy CT pulmonary angiography, and radiation dose considerations.
Conflict of interest statement
Figures




References
-
- Tapson VF. Acute pulmonary embolism. N Engl J Med. 2008;358:1037–1052. - PubMed
-
- Victoria T, Mong A, Altes T, et al. Evaluation of pulmonary embolism in a pediatric population with high clinical suspicion. Pediatr Radiol. 2009;39:35–41. - PubMed
-
- Kritsaneepaiboon S, Lee EY, Zurakowski D, et al. MDCT pulmonary angiography evaluation of pulmonary embolism in children. AJR Am J Roentgenol. 2009;192:1246–1252. - PubMed
-
- Zhang LJ, Zhang Z, Li SJ, et al. Pulmonary embolism and renal vein thrombosis in patients with nephrotic syndrome: prospective evaluation of prevalence and risk factors with CT. Radiology. 2014;273:897–906. - PubMed
Publication types
MeSH terms
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
