

Vulvar cancer: epidemiology, clinical presentation, and management options
- PMID: 25848321
- PMCID: PMC4374790
- DOI: 10.2147/IJWH.S68979
Vulvar cancer: epidemiology, clinical presentation, and management options
Abstract
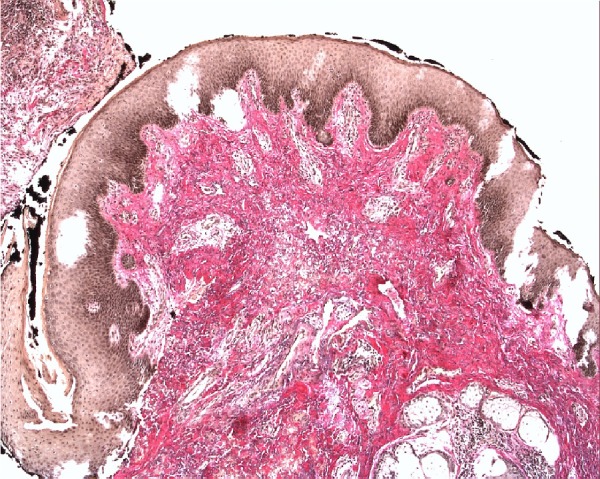
Epidemiology: Vulvar cancer can be classified into two groups according to predisposing factors: the first type correlates with a HPV infection and occurs mostly in younger patients. The second group is not HPV associated and occurs often in elderly women without neoplastic epithelial disorders.
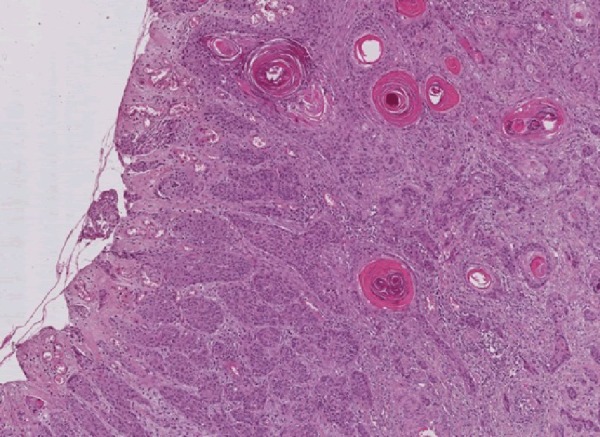
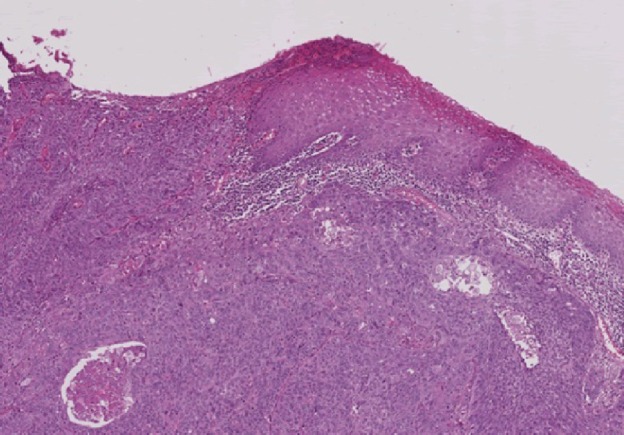
Histology: Squamous cell carcinoma (SCC) is the most common malignant tumor of the vulva (95%).
Clinical features: Pruritus is the most common and long-lasting reported symptom of vulvar cancer, followed by vulvar bleeding, discharge, dysuria, and pain.
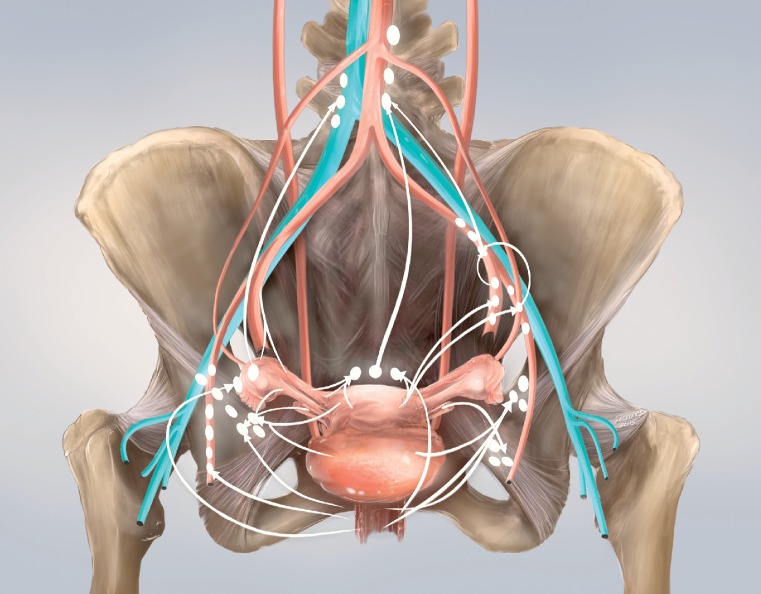
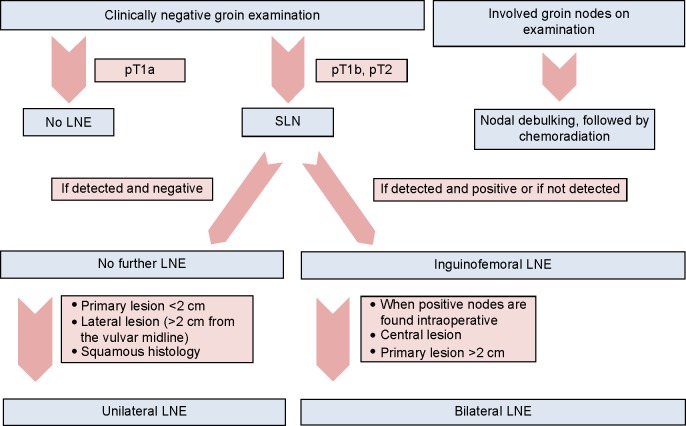
Therapy: The gold standard for even a small invasive carcinoma of the vulva was historically radical vulvectomy with removal of the tumor with a wide margin followed by an en bloc resection of the inguinal and often the pelvic lymph nodes. Currently, a more individualized and less radical treatment is suggested: a radical wide local excision is possible in the case of localized lesions (T1). A sentinel lymph node (SLN) biopsy may be performed to reduce wound complications and lymphedema.
Prognosis: The survival of patients with vulvar cancer is good when convenient therapy is arranged quickly after initial diagnosis. Inguinal and/or femoral node involvement is the most significant prognostic factor for survival.
Keywords: HPV infection; groin dissection; overall survival; radical vulvectomy; sentinel lymph node biopsy; vulvar cancer.
Figures
References
-
- Siegel R, Naishadham D, Jemal A. Cancer statistics, 2013. CA Cancer J Clin. 2013;63(1):11–30. - PubMed
-
- Hunter DJ. Carcinoma of the vulva: a review of 361 patients. Gynecol Oncol. 1975;3(2):117–123. - PubMed
-
- Horn LC, Klostermann K, Hautmann S, Höhn AK, Beckmann MW, Mehlhorn G. HPV-assoziierte Veränderungen an Vulva und Vagina [HPV-associated alterations of the vulva and vagina. Morphology and molecular pathology] Pathologe. 2011;32(6):467–475. German. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Research Materials
