

Hepatitis C virus syndrome: A constellation of organ- and non-organ specific autoimmune disorders, B-cell non-Hodgkin's lymphoma, and cancer
- PMID: 25848462
- PMCID: PMC4381161
- DOI: 10.4254/wjh.v7.i3.327
Hepatitis C virus syndrome: A constellation of organ- and non-organ specific autoimmune disorders, B-cell non-Hodgkin's lymphoma, and cancer
Abstract
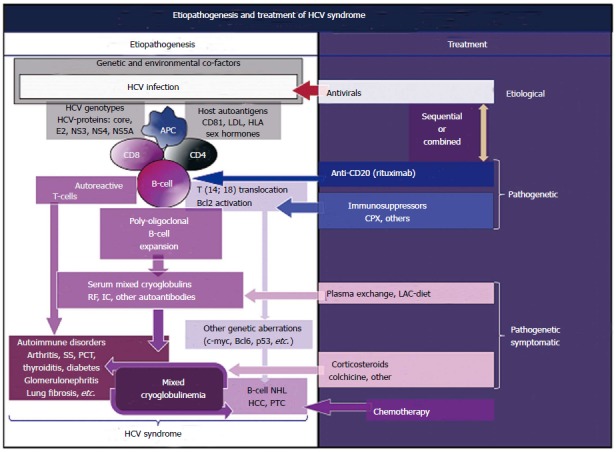
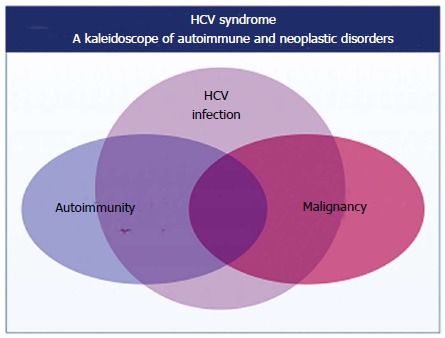
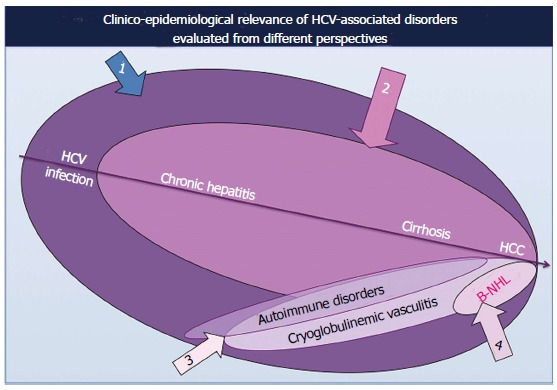
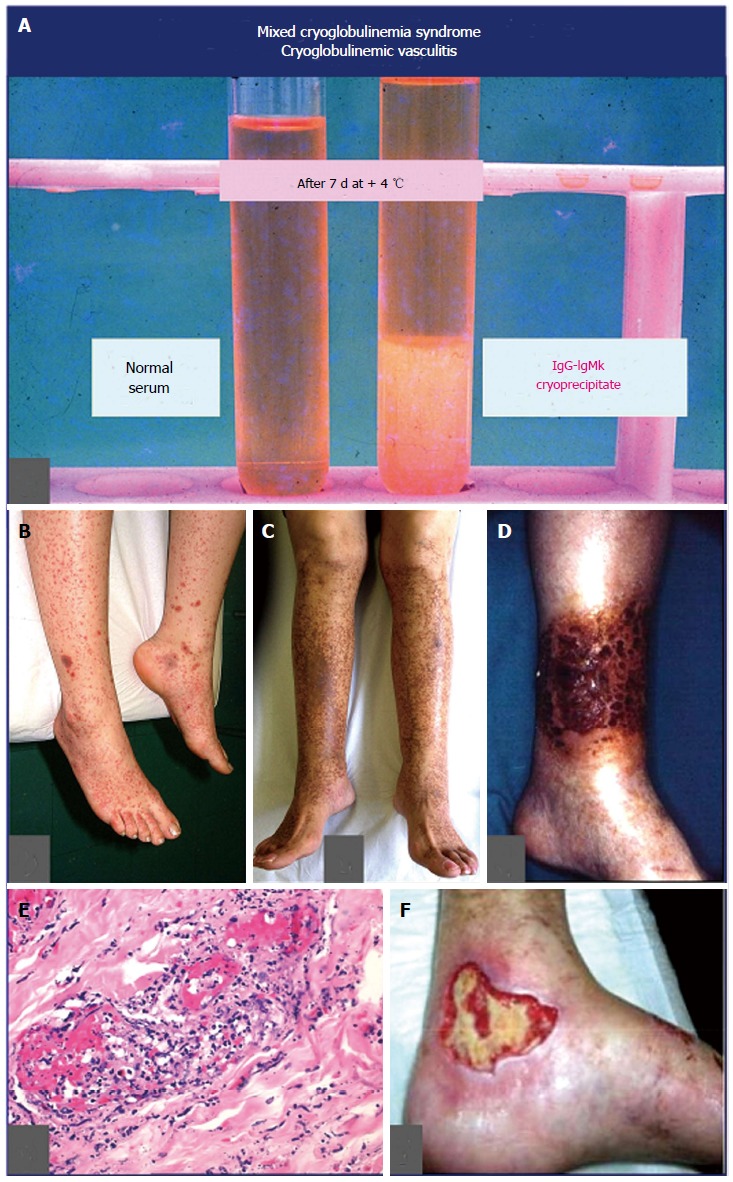
The clinical course of chronic hepatitis C virus (HCV) infection is characterized by possible development of both liver and extrahepatic disorders. The tropism of HCV for the lymphoid tissue is responsible for several immune-mediated disorders; a poly-oligoclonal B-lymphocyte expansion, commonly observed in a high proportion of patients with HCV infection, are responsible for the production of different autoantibodies and immune-complexes, such as mixed cryoglobulins. These serological alterations may characterize a variety of autoimmune or neoplastic diseases. Cryoglobulinemic vasculitis due to small-vessel deposition of circulating mixed cryoglobulins is the prototype of HCV-driven immune-mediated and lymphoproliferative disorders; interestingly, in some cases the disease may evolve to frank malignant lymphoma. In addition, HCV shows an oncogenic potential as suggested by several clinico-epidemiological and laboratory studies; in addition to hepatocellular carcinoma that represents the most frequent HCV-related malignancy, a causative role of HCV has been largely demonstrated in a significant percentage of patients with isolated B-cells non-Hodgkin's lymphomas. The same virus may be also involved in the pathogenesis of papillary thyroid cancer, a rare neoplastic condition that may complicate HCV-related thyroid involvement. Patients with HCV infection are frequently asymptomatic or may develop only hepatic alteration, while a limited but clinically relevant number can develop one or more autoimmune and/or neoplastic disorders. Given the large variability of their prevalence among patients' populations from different countries, it is possible to hypothesize a potential role of other co-factors, i.e., genetic and/or environmental, in the pathogenesis of HCV-related extra-hepatic diseases.
Keywords: Diabetes; Hepatitis C virus; Lymphoma; Mixed cryoglobulinemia; Thyroid.
Figures
References
-
- Choo QL, Kuo G, Weiner AJ, Overby LR, Bradley DW, Houghton M. Isolation of a cDNA clone derived from a blood-borne non-A, non-B viral hepatitis genome. Science. 1989;244:359–362. - PubMed
-
- Ferri C, Marzo E, Longombardo G, Lombardini F, Greco F, Bombardieri S. Alpha-interferon in the treatment of mixed cryoglobulinemia patients. International Cancer Update. Focus on Interferon Alfa 2b. Cannes, France. November 1-4, 1990. Eur J Cancer. 1991;27:81–82. - PubMed
-
- Pascual M, Perrin L, Giostra E, Schifferli JA. Hepatitis C virus in patients with cryoglobulinemia type II. J Infect Dis. 1990;162:569–570. - PubMed
-
- Meltzer M, Franklin EC, Elias K, McCluskey RT, Cooper N. Cryoglobulinemia--a clinical and laboratory study. II. Cryoglobulins with rheumatoid factor activity. Am J Med. 1966;40:837–856. - PubMed
Publication types
LinkOut - more resources
Full Text Sources
Other Literature Sources
