

Bone microdamage, remodeling and bone fragility: how much damage is too much damage?
- PMID: 25848533
- PMCID: PMC4371415
- DOI: 10.1038/bonekey.2015.11
Bone microdamage, remodeling and bone fragility: how much damage is too much damage?
Abstract
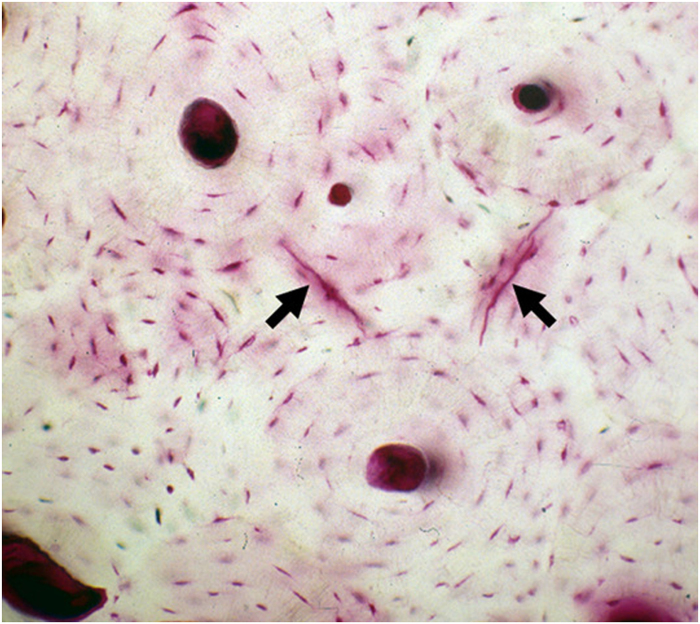
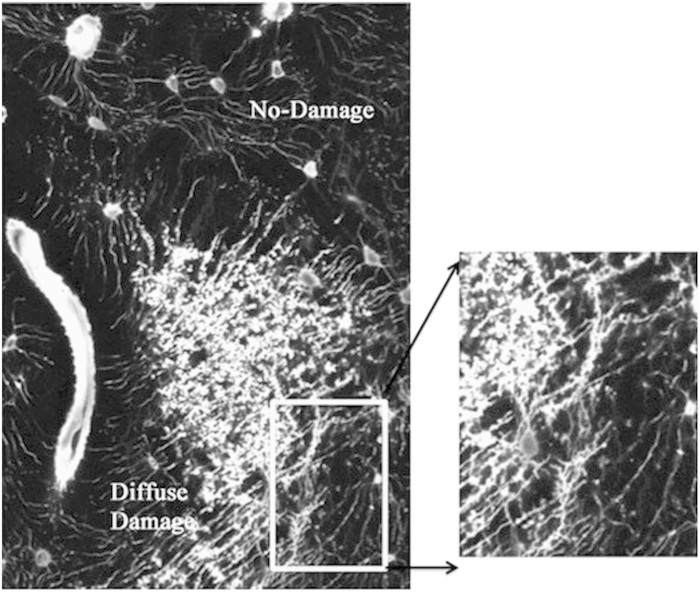
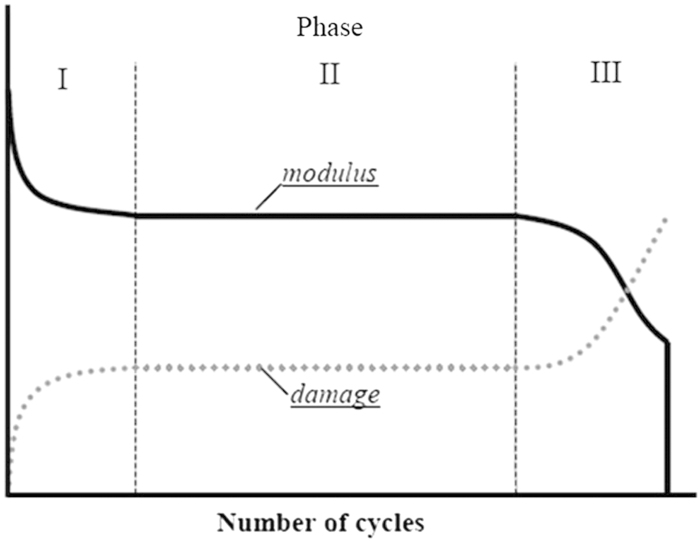
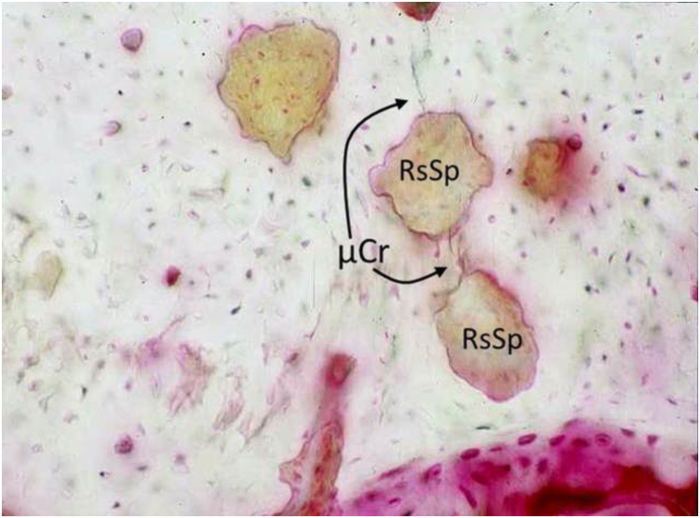
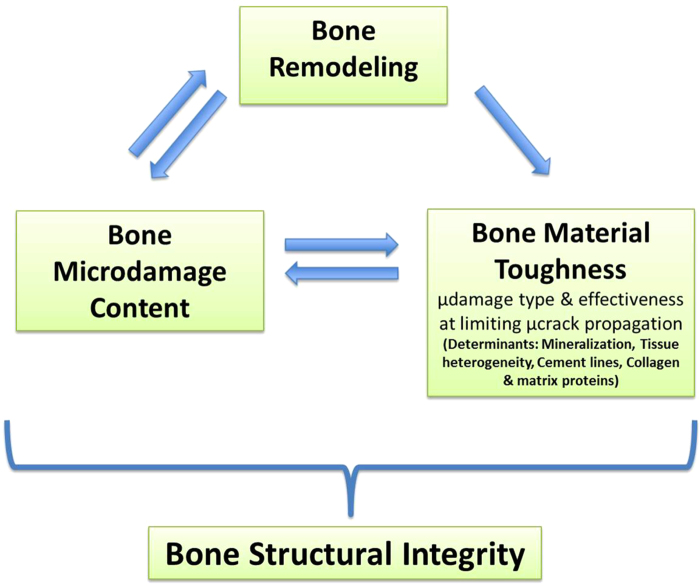
Microdamage resulting from fatigue or 'wear and tear' loading contributes to bone fragility; however, the full extent of its influence is not completely understood. Linear microcracks (∼50-100 μm) and diffuse damage (clusters of sublamellar-sized cracks) are the two major bone microdamage types, each with different mechanical and biological consequences. Healthy bone, due to its numerous microstructural interfaces and its ability to affect matrix level repair, deals effectively with microdamage. From a material standpoint, healthy bone behaves much like engineering composites like carbon-fiber reinforced plastics. Both materials allow matrix damage to form during fatigue loading and use microstructural interfaces to dissipate energy and limit microcrack propagation to slow fracture. The terms fracture toughness and 'toughening mechanism', respectively, describe mechanical behavior and microstructural features that prevent crack growth and make it harder to fracture a material. Critically, toughness is independent of strength. In bone, primary toughening features include mineral and collagen interfaces, lamellae and tissue heterogeneity among osteons. The damage tolerance of bone and other composites can be overcome with sustained loading and/or matrix changes such that the microstructure no longer limits microcrack propagation. With reduced remodeling due to aging, disease or remodeling suppression, microdamage accumulation can occur along with loss of tissue heterogeneity. Both contribute additively to reduced fracture toughness. Thus, the answer to the key question for bone fragility of how much microdamage is too much is extremely complex. It ultimately depends on the interplay between matrix damage content, internal repair and effectiveness of matrix-toughening mechanisms.
Figures
References
-
- Osteoporosis in the workplace: the social, economic and human costs of osteoporosis on employees, employers and governments. Prepared by the World Health Organization Collaborating Center, Liege, Belgium on behalf of the IOF Committee of Scientific Advisors. Available at http://www.iofbonehealth.org, 2002.
-
- Becker DJ, Kilgore ML, Morrisey MA. The societal burden of osteoporosis. Curr Rheumatol Rep 2010; 12: 186–191. - PubMed
-
- Vashishth D. Rising crack-growth-resistance behavior in cortical bone: implications for toughness measurements. J Biomech 2004; 37: 943–946. - PubMed
-
- Burr DB, Forwood MR, Fyhrie DP, Martin RB, Schaffler MB, Turner CH. Bone microdamage and skeletal fragility in osteoporotic and stress fractures. J Bone Miner Res 1997; 12: 6–15. - PubMed
Publication types
Grants and funding
LinkOut - more resources
Full Text Sources
Other Literature Sources