

Invasive lobular carcinoma of the breast: morphology, biomarkers and 'omics
- PMID: 25849106
- PMCID: PMC4310190
- DOI: 10.1186/s13058-015-0519-x
Invasive lobular carcinoma of the breast: morphology, biomarkers and 'omics
Abstract
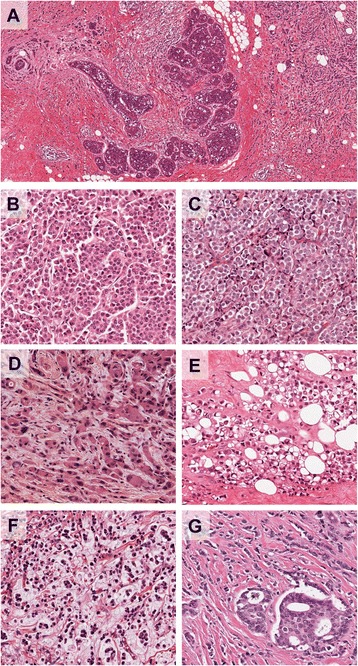
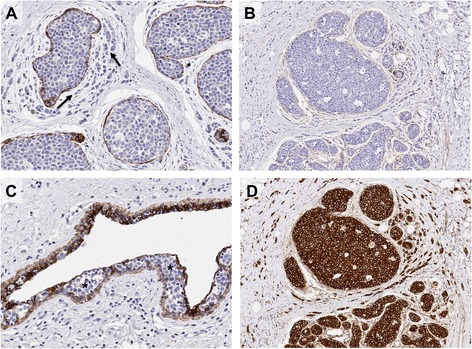
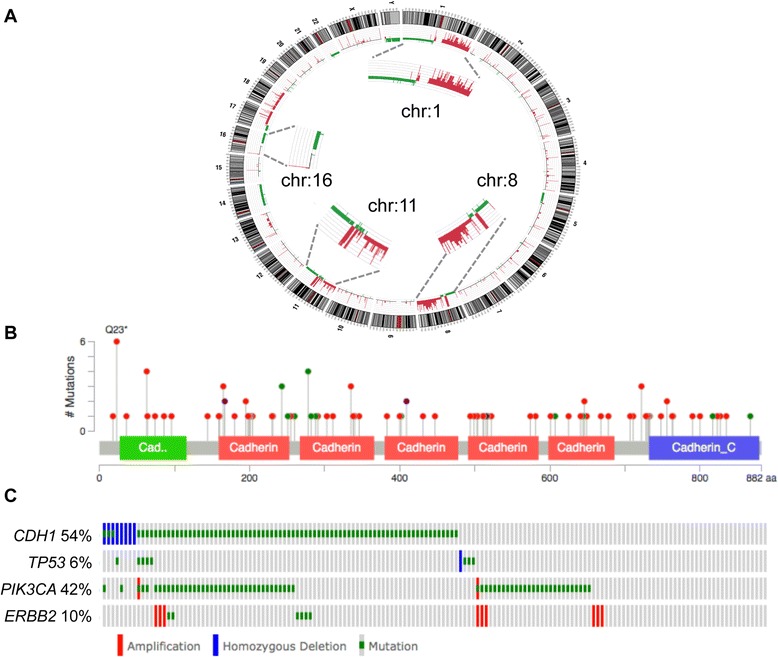
Invasive lobular carcinoma of the breast is the most common 'special' morphological subtype of breast cancer, comprising up to 15% of all cases. Tumours are generally of a good prognostic phenotype, being low histological grade and low mitotic index, hormone receptor positive and HER2, p53 and basal marker negative, and with a generally good response to endocrine therapy. Despite this, clinicians face countless challenges in the diagnosis and long-term management of patients, as they encounter a tumour that can be difficult to detect through screening, elicits a very invasive nature, a propensity for widespread metastatic colonisation and, consequently, in some studies a worse long-term poor outcome compared with invasive carcinoma of no special type. Here we review the morphological and molecular features that underpin the disparate biological and clinical characteristics of this fascinating tumour type.
Figures
References
-
- Pestalozzi BC, Zahrieh D, Mallon E, Gusterson BA, Price KN, Gelber RD, Holmberg SB, Lindtner J, Snyder R, Thurlimann B, Murray E, Viale G, Castiglione-Gertsch M, Coates AS, Goldhirsch A, International Breast Cancer Study Group Distinct clinical and prognostic features of infiltrating lobular carcinoma of the breast: combined results of 15 International Breast Cancer Study Group clinical trials. J Clin Oncol. 2008;26:3006–14. doi: 10.1200/JCO.2007.14.9336. - DOI - PubMed
-
- Lakhani SR, Ellis IO, Schnitt SJ, Tan PH, van de Vijver MJ. WHO Classification of Tumours of the Breast. 4. Lyon: IARC; 2012.
Publication types
MeSH terms
Substances
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Research Materials
Miscellaneous
