

The use of autologous fascia lata graft in the laparoscopic reinforcement of large hiatal defect: initial observations of the surgical technique
- PMID: 25849293
- PMCID: PMC4359456
- DOI: 10.1186/s12893-015-0008-2
The use of autologous fascia lata graft in the laparoscopic reinforcement of large hiatal defect: initial observations of the surgical technique
Abstract
Background: Even though there is no consensus, many authors believe that in the cases of large hiatal defects, structurally altered crura and/or absence of peritoneal lining, a crural reinforcement should be performed. Reinforcement could be performed with different techniques and different type of mesh, either synthetic or biologic. The disadvantages of mesh repair include the possibility of serious complications and increased costs especially in the usage of composite or biologic mesh.
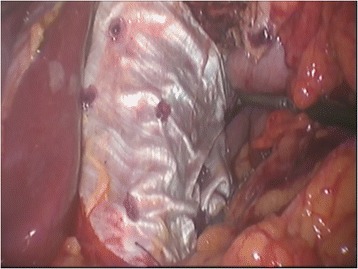
Methods: The study includes 10 cases of reinforced primary suture line of the pillars with autologous fascia lata, in elective laparoscopic repair of the giant PEH with a large hiatal defect and friable crura. After intraopreative confirmation of the large hiatal defect (hiatal surface area of more than 8 cm²) and friable crura, an autologous fascia lata graft was harvested in the usual manner and placed in on-lay fashion to reinforce the pillar suture line. We analyzed surgical technique, complications, and initial follow-up of the patients.
Results: Average hiatal surface area (HSA) in our series was 10.6 cm² (range 8.1 to 14.4 cm²). The average duration of operation was 203.9 min/3.4 hours (range 160-250 min). Except for a mild hematoma in the harvesting region that resolved spontaneously, there were no procedure related complications and 30 days mortality rate was zero. The average postoperative length of stay was 6.5 days (5-8 days). Out of 10 patients, 5 completed the annual follow-up visit, while 8 completed a 6- month follow-up visit. So far there is no hernia recurrence and/or problems with swallowing function. However, one patient has felt a mild discomfort in the harvested region that does not influence normal daily activities.
Conclusions: Autologous fascia lata graft hiatal reinforcement represents a technically feasible, easy, and available option for the on-lay reinforcement of large hiatal defects with friable crura in the laparoscopic repair of giant PEHs.
Figures

References
MeSH terms
LinkOut - more resources
Full Text Sources
Other Literature Sources
Medical
Miscellaneous
